Cochlear implantation (CI) is the standard treatment for patients with severe to profound sensorineural hearing loss (HL), for which hearing aids are not beneficial [1-3]. The complications after CI are classified as minor or major, and major complications usually necessitate revision surgery [4]. Electrode array extrusion or migration is rare, but it is a major complication that requires re-implantation and accounts for 1%–15% of all revision operations for CI [4,5]. The incidence of electrode extrusion or migration in CI has been reported to range between 1% and 12% [6]. Considering the significance of electrode extrusion in CI, in this study, we reviewed and analyzed several patients who experienced electrode array extrusion of CI to obtain a fuller understanding of the risks and mechanisms of electrode extrusion in CI.
The Institutional Review Board of Severance Hospital approved this study (IRB No. 4-2021-1400) and written informed consent was waived. We retrospectively reviewed the medical records of 1,391 patients with CI at our tertiary institution from October 1988 to December 2020. Among these patients, we identified seven patients who experienced electrode extrusion (Table 1). There were six male patients and one female patient, one individual of pediatric age and six adults. The pediatric patient who had CI had congenital HL, and the six adult patients with CI had a history of mastoidectomy due to chronic otitis media (COM) before CI. Among the patients in whom mastoidectomy was performed, five patients underwent open cavity (canal wall down) mastoidectomy, and one underwent intact canal wall (canal wall up) mastoidectomy.
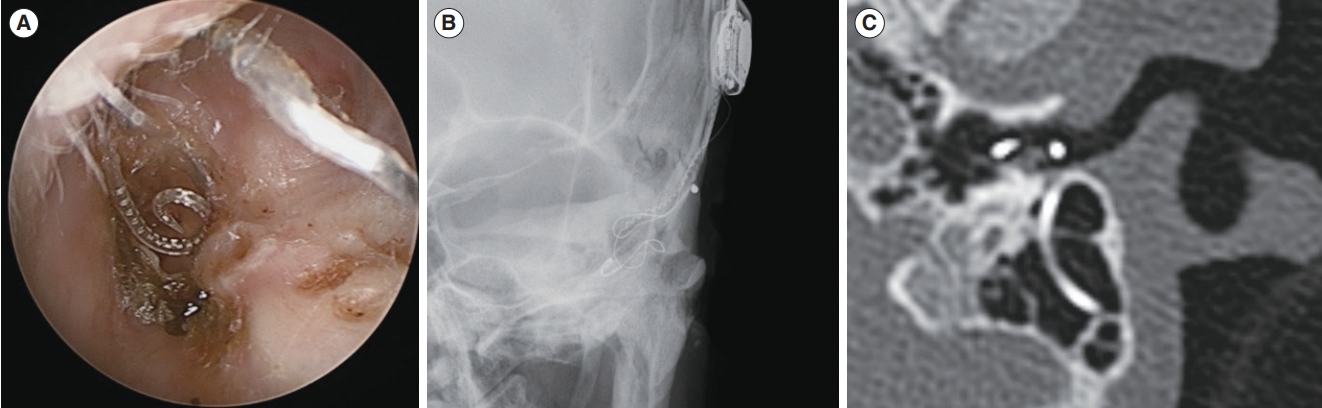
The extruded electrode arrays were straight-type in four patients and perimodiolar-type in three patients. The mean interval between CI and electrode extrusion was 8.6±5.5 years (range, 11 months–14 years 11 months). Regarding the events before electrode extrusion, high impedance was measured at four channels in one pediatric patient, and HL was aggravated after ear wax removal, ear pick use, inflammation, or ear dressing in four adult patients. There were no specific events in the other two adult patients. Electrode extrusion was confirmed by a physical examination at an outpatient clinic and a transocular plain X-ray or temporal bone computed tomography in all patients. The electrode arrays were extruded from the cochlea and exposed in the external auditory canal (EAC) in all patients. The posterior EAC exhibited destruction in two patients with a previously intact EAC, and no new bone formation was observed in the pediatric patient (Fig. 1). The devices were removed from all seven patients, and simultaneous revision CI was performed in four patients.
During surgery for CI in six patients with previous mastoidectomy and for revision CI in four patients, the remnant air cells in mastoid bone were drilled out to avoid an aggravated infection. The inserted electrode was covered sufficiently with temporalis fascia, cartilage, and fibrin glue along the full length. We did not perform subtotal petrosectomy in these patients considering the disadvantages of that procedure, such as EAC blind sac closure breakdown, entrapped cholesteatoma, and infection of the obliterated cavity.
Electrode extrusion should be considered in patients with open cavity mastoidectomy. Mastoid cavities in patients with canal wall down mastoidectomy raise concerns with operative and postoperative management, especially when there is a large meatoplasty. Several surgical techniques to reduce operative and postoperative complications in these patients have been reported, including maintenance of the cavity with soft tissue coverage of the electrode, overclosure of the EAC with and without mastoid obliteration or Eustachian tube plugging, posterior EAC wall reconstruction, subtotal petrosectomy with EAC overclosure, and CI via the middle fossa approach bypassing the canal wall down cavity [7]. Subtotal petrosectomy with closure of the EAC was reported to be an appropriate method for CI in patients with COM [1,3,8,9].
The mechanism of electrode migration remains unclear [4,5]. However, several mechanisms of electrode extrusion have been described. Iatrogenic defects of the posterior EAC during CI were reported to be the cause of electrode extrusion. If an electrode is in contact with the posterior EAC wall, pressure on the wall could have an effect on wall breakdown, particularly if the wall is excessively thinned [10]. Head trauma and intracochlear fibrosis and ossification can induce electrode extrusion [4,5]. In the present study, four of the six adult patients had events of traumatic external force or inflammation in the implanted ear before electrode extrusion. Based on our study and previous reports, previous mastoidectomy can be a risk factor for electrode extrusion due to a posterior EAC wall defect or thinning.
For CI in children, new bone formation and mastoid growth are mechanisms of electrode extrusion. The electrode array might be fixed by new bone formation at the mastoid tip. New bone formation within the mastoid cavity during skull growth can displace the electrode over time, pulling it out of the cochlea [4,5]. Straight electrodes have a higher incidence of extrusion than perimodiolar electrodes due to their design. Precurved perimodiolar electrode arrays can be self-retained inside the cochlea, whereas straight electrode arrays can exert forces on the cochlear outer wall due to their inherent tendency to spring back into their original straight position [5,6]. However, in the present study, three of the seven patients with electrode extrusion had received perimodiolar electrode arrays.
In a study by Dietz et al. [5] with 162 patients with CI, 12 patients with CI electrode extrusion were identified and all extruded electrodes were straight. In another systematic review, the interval between CI and electrode migration ranged from weeks to several years [4]. In the present study, the mean interval between CI and electrode extrusion was longer in patients with perimodiolar electrode arrays (55.3±5.51 months) than in those with straight electrode arrays (36.4±22.9 months). Therefore, although straight electrodes have a higher risk of extrusion than perimodiolar electrodes, perimodiolar electrodes can be extruded long after CI.
We verified the relatively high risk of electrode extrusion in adult patients with open cavity mastoidectomy and in pediatric patients based on long-term experience. Canal wall down mastoid cavity and young age in pediatric patients are risk factors for electrode array extrusion in CI. Patients with these factors should be followed long-term to assess electrode extrusion.