INTRODUCTION
Spontaneous pneumomediastinum and pneumothorax commonly occur in healthy young men or parturient women, in whom increased intra-alveolar pressure (Valsalva maneuver, cough, emesis) leads to the rupture of marginal pulmonary alveoli (1). In contrast, pneumomediastinum and pneumothorax following cervical emphysema are very rare and few case reports have been published. However, they have been reported in relation to dental surgical procedures, head and neck surgery, or orofacial trauma. In thyroid surgery, pneumothorax and pneumomediastinum are usually associated with difficult dissection toward the pleura or mediastinum (2). We review one case of pneumomediastinum and pneumothorax following cervical emphysema after thyroid surgery without mediastinal dissection and pleural injury.
CASE REPORT
A 60-year-old woman admitted for elective excision of a right thyroid papillary carcinoma. She had complained of hoarseness and aspiration while swallowing for several months. Rigid endoscopy confirmed paramedian vocal cord fixation with large glottic chink. Preoperative computed tomography (CT) detected a solid thyroid mass invading the perithyroid tissue with suspicion of right tracheoesophageal groove invasion. Total thyroidectomy with central neck dissection was carried out via transcervical incision. Intraoperatively, the tumor was found to invade the right recurrent laryngeal nerve and along the right tracheoesophageal groove (Fig. 1A). The right recurrent laryngeal nerve was sacrificed and the tumor invading the tracheoesophageal groove was shaved off the trachea and esophagus. After tracheal shaving, a small perforation (0.5├Ś0.5 cm) was noticed in the posterior membranous portion of first tracheal ring (Fig. 1B). The pleura of the lung and mediastinum were intact. The perforation was repaired primarily with No. 4-0 Vicryl suture and reinforced with Surgicel┬« and tissue glue. The trachea did not leak by underwater testing during positive anesthetic ventilation and the operation was completed.
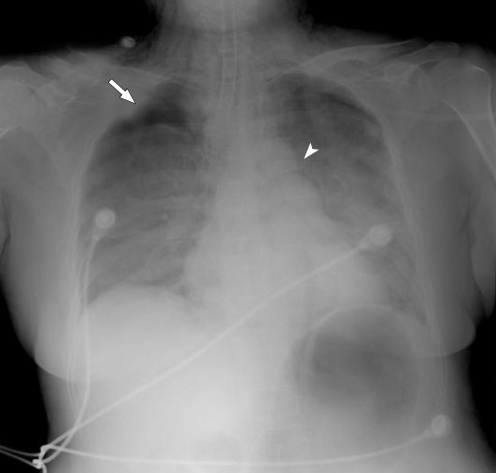
One day after surgery, the patient developed dyspnea, cervical emphysema, and ecchymosis over the neck after an episode of vigorous coughing. With the impression of a postoperative hematoma an emergency neck exploration was performed under general anesthesia. A small hematoma was found beneath the platysma and strap muscles, No obvious bleeding point was evident and the reconstructed trachea portion was relatively intact. Postoperatively, while still in the recovery room, the patient showed signs of acute respiratory failure. A chest radiograph revealed bilateral pneumothorax, pneumomediastinum, and massive subcutaneous emphysema (Fig. 2). Her dyspnea and cyanosis were relieved after an emergency chest tube was inserted. Over the next week, the pneumomediastinum and pneumothorax resolved gradually. The patient discharged without any problems.
DISCUSSION
Pneumomediastinum and pneumothorax are defined as the presence of air in the mediastinum and thoracic cavity, respectively. Air may gain access to the mediastinum and thoracic cavity through several anatomic routes: directly, through a perforation of the trachea, bronchi, or esophagus; by dissection along the fascial planes of the neck; from the interstitial tissue of the lung; or from the retroperitoneal space (1). In most cases of pneumothorax and pneumomediastinum, air ascends along the mediastinum toward the subcutaneous space of the neck after rupture of marginal pulmonary alveoli. In contrast, pneumothorax and pneumomediastinum following cervical emphysema are very rare.
In thyroid surgery, pneumothorax and pneumomediastinum are usually associated with a difficult dissection toward the pleura or mediastinum. As a result, postoperative pneumothorax can be encountered. The most likely scenario is that air tracks through the cervical fascial planes under low pressure or that the pleura is violated inadvertently. Nevertheless, the resulting pneumothorax or pneumomediastinum are usually of little clinical importance (2). However, they can be associated with several serious complications including cardiac tamponade, tension pneumomediastinum, air embolism, mediastinitis and neck abscess (3). In this patient, pneumothorax, and pneumomediastinum occurred through a minor tracheal perforation around the tracheoesophageal groove after tracheal shaving, despite preservation of intact pleura of the lung and mediastinum.
Initially, dyspnea was considered as a consequence of airway compression due to postoperative hematoma. However, after thorough review of the patient's hospital course, we speculate that she had already developed pneumomediastinum and pneumothorax prior to our exploration of the neck.
The mechanisms of her pneumothorax may be as follows. First, postoperative hematoma and narrowed airway from medially fixed unilateral vocal fold aggravate dyspnea. Second, a high-pressure air leak occurred through the perforated trachea due to deep breathing and vigorous coughing. Finally, along the fascial planes of the neck, pneumomediastinum and bilateral tension pneumothorax occurred before neck exploration. Consistent with this route, air leak can be aggravated by tracheal injury during intubation and by positive-pressure ventilation anesthesia during a subsequent operation.
There are two possisle points of inadvertent tracheal injury exists: one is at freeing the isthmus from the trachea and the other at dissecting the lateral and posterior aspect of the trachea close to the area where the recurrent laryngeal nerve enters the tracheal cartilage (4). Although secondary complications such as subcutaneous emphysema, pneumothorax and pneumomediastinum may occur very rarely, most patients recover without any problems with primary tracheal repair. Repair of tracheal perforations usually performed by re-approximating the tracheal edges with an absorble suture, and sometimes reinforced by adjacent strap muscle flaps using fibrin glue (5).