INTRODUCTION
Chronic rhinosinusitis (CRS) is one of the main causes of olfactory dysfunction, accounting for 15%-30% of cases involving loss of smell [1-3]. Olfactory dysfunction in CRS usually improves subjectively and/or objectively after surgery in long term follow-up (Ōēź6 months). However, the improvement rate is widely variable, from no improvement to 97% [4-10]. This diverse improvement rate may reflect the use of different kinds of olfactory tests, follow-up periods, and study populations. Edema and granulation tissue may be the cause of bad results in short-term follow-up (<6 months) studies. Similarly, scar formation, recurrent disease, and new polyp formation in the region of the olfactory cleft can also affect postoperative results in long-term follow-up (Ōēź6 months) studies [4]. Therefore, postoperative wound healing status may be one of important factors in the analyses of olfactory function after endoscopic sinus surgery (ESS).
The present study analyzed postoperative results according to wound healing status in CRS with nasal polyps (NP). In addition, the clinical characteristics of subjects with favorable wound healing but no improvement of olfaction, who clinicians may often face, were analyzed.
MATERIALS AND METHODS
Subjects
Thirty out of this study population have been previously reported and this is add-on study to previous publication that correlated preoperative findings on computed tomography (CT) with poor olfactory outcome [11]. Fifty subjects, who were diagnosed with CRS and NP with a smelling disturbance and were treated with ESS, were enrolled in this study.
Frontoethmoidectomy with middle meatal antrostomy (with/without sphenoidectomy) was performed in all cases. Surgery in the olfactory cleft and middle turbinectomy were not performed. Preoperative steroids were not given and nasal steroid spray or antibiotics were used on the all subjects for 1-3 months after surgery.
The diagnosis was based on at least a 3-month history of rhinosinusitis, findings of nasal endoscopy, CT findings, and olfactory function tests. Patients were excluded if they had a history of head trauma, acute olfactory dysfunction after previous upper respiratory tract infection, age <15 or >65 years, history of previous sinus surgery, and combined septoturbinoplasty. All patients filled out questionnaires and underwent the butanol threshold test (BTT) and the cross-cultural smell identification test (CCSIT) at the initial preoperative visit and at 6 months after surgery.
An endoscopic examination had been performed by one investigator blinded to study design before postoperative olfactory tests were conducted. Pathological findings, including discharge, edema, and polyp in the nasal cavity were checked. According to the Lund-Kennedy score [12], subjects were divided into two groups: favorable wound healing group, who was scored 0, and unfavorable wound healing group, who showed pathologic findings. Unfavorable group was divided according to score: mild group who was scored 1-6 and severe group who was scored 7-12. This study was approved by the Institutional Review Board of Gyeongsang National University Hospital.
Ostiomeatal unit CT
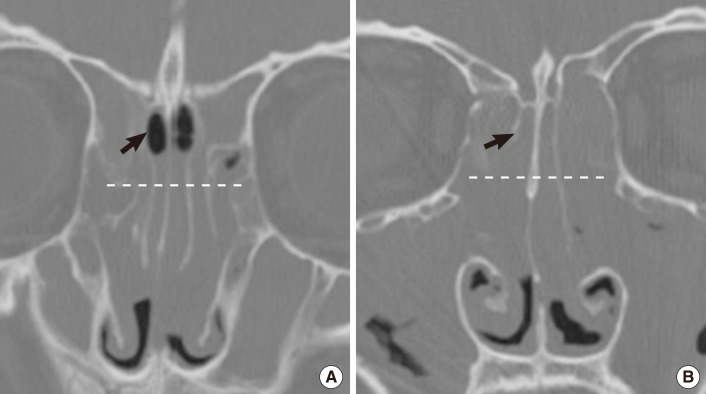
The preoperative ostiomeatal unit (OMU) CT images at 2.5 mm thickness were evaluated in the axial and coronal planes without contrast enhancement. All of the paranasal sinuses were graded on a scale of 0-2 according to the Lund-Mackay system [13]. CT grading of olfactory cleft opacification was done as previously reported [11]. CT grading was performed by one investigator blinded to this study design. The borders of the olfactory cleft were defined as follows. The anterior, posterior, medial, and lateral borders were the anterior attachment of the middle turbinate, anterior wall of the sphenoid sinus, nasal septum, and middle and superior turbinates, respectively. The superior border was the skull base. The inferior border was the inferior portion of the middle turbinate. We divided the olfactory cleft into two parts: anterior olfactory cleft and posterior olfactory cleft, which were split by the anterior end of the superior turbinate. In addition, the olfactory cleft was divided into upper and lower parts, which were split by imaginary midline (Fig. 1). The adoption of the grading of upper part of the olfactory cleft was because these areas are the true sensory cavity [14]. Each olfactory cleft opacification was graded on a scale of 0-4 via the ratio of the opacified area to the whole area of the olfactory cleft (0, no opacification; 1, Ōēż25%; 2, 25%-50%; 3, 50%-75%; 4, >75%).
Olfactory function tests
The odor threshold was determined using the BTT. Four percent N-butanol (Sigma-Aldrich, St Louis, MO, USA) was serially diluted 3-fold with mineral oil (Sigma-Aldrich) to form a series of 10 concentrations. The test was performed in each nostril separately. The examinees were given two polyethylene bottles, one with mineral oil and the other with butanol. The patients were asked to choose the bottle with butanol. The test was repeated until the butanol bottle was correctively identified by the examinee in five consecutive trials. The examination was started at concentration level of 10. The concentration level was designated as the threshold level. For the BTT, anosmia was defined as concentration levels of 0-1, severe hyposmia as levels 2-3, moderate hyposmia as levels 4-5, mild hyposmia as levels 6-7, and normosmia as levels 8-9 [15].
To test odor identification, the CCSIT (Sensonics, Haddon Heights, NJ, USA) was performed in both nostrils simultaneously. The threshold of the CCSIT was defined as the mean odor threshold of both nostrils. Anosmia was defined as concentration levels 0-3, severe hyposmia as levels 4-5, moderate hyposmia as levels 6-8, mild hyposmia as levels 9-10, and normosmia as levels 11-12 [16].
The validated questionnaire including 14 odors common in Korea was performed in the presence of a trained research coordinator. Patients were asked to grade their olfactory dysfunction on a scale of 0-4, with 0 being a normal sense of smell to 4 being complete anosmia. The correlation between the responses to the questionnaire and objective tests was validated as described previously [17]. Postoperative success rate was classified as complete success (improvement of all olfactory tests), partial success (improvement of at least two olfactory tests), and others (failure).
Statistical analyses
Statistical analyses were performed with SPSS ver. 18.0 (SPSS Inc., Chicago, IL, USA). The Student's t-test (or Mann-Whitney U test) or Žć2-test (or Fisher's exact test) were applied to determine statistical differences (P<0.05). Data was expressed as the mean┬▒standard deviation (SD).
RESULTS
Demographic data and baseline characteristics of subjects
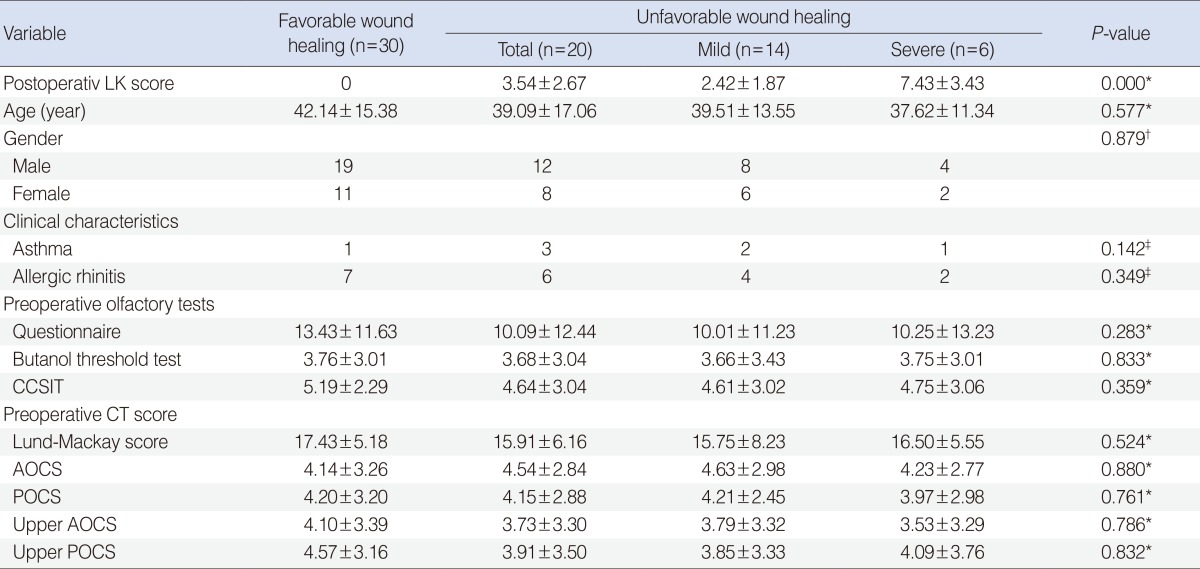
There were 31 male and 19 female patients. The ages ranged from 16 to 63 years (mean, 40.8 years). Preoperative questionnaire, BTT and CCSIT scores averaged 12.06┬▒12.18, 3.73┬▒2.90, and 5.39┬▒2.78, respectively. Preoperative Lund-Mackay score, anterior olfactory cleft score (AOCS), posterior olfactory cleft score (POCS), upper AOCS, and upper POCS was 16.82┬▒5.17, 4.29┬▒3.08, 4.18┬▒3.15, 3.95┬▒3.14, and 4.30┬▒3.17, respectively. In terms of postoperative wound healing status, demographic data and associated medical history are shown in Table 1. There were no differences in demographics, preoperative olfactory tests, and preoperative CT findings.
Comparison of postoperative olfactory results according to wound healing status
For favorable wound healing group (n=30), the mean improvement of questionnaire, BTT, and CCSIT were 19.70┬▒14.31, 2.88┬▒2.55, and 2.24┬▒2.74, respectively. Improvement rates of questionnaire, BTT and CCSIT were 90%, 83%, and 63%, respectively. All patients with improved BTT also showed improved questionnaire responses. Among the 20 patients with improved CCSIT, postoperative BTT and questionnaire improved in 19 patients. There was only one case of isolated improvement of CCSIT. Nineteen out of 30 patients (63%) showed complete success, followed by 20% partial success (n=6). Five subjects (16%) were included in the failure criteria.
For the unfavorable wound healing group (n=20), the mean improvement of questionnaire, BTT, and CCSIT scores were 11.38┬▒17.06, 1.23┬▒3.38, and 0.62┬▒3.25, respectively. Improvement rates of questionnaire, BTT, and CCSIT were 60%, 45%, and 25%, respectively. Twelve out of 20 patients (60%) were classified as failure. Five subjects (25%) and three subjects (15%) were classified as complete success and partial success, respectively. Subjects in the favorable wound healing group showed more marked mean improvement of olfactory results, improvement and success rates than the unfavorable wound healing group. Mild group showed higher mean improvement of olfactory results than severe group in the unfavorable group (Table 2).
Preoperative clinical characteristics according to postoperative olfactory results in the favorable wound healing group
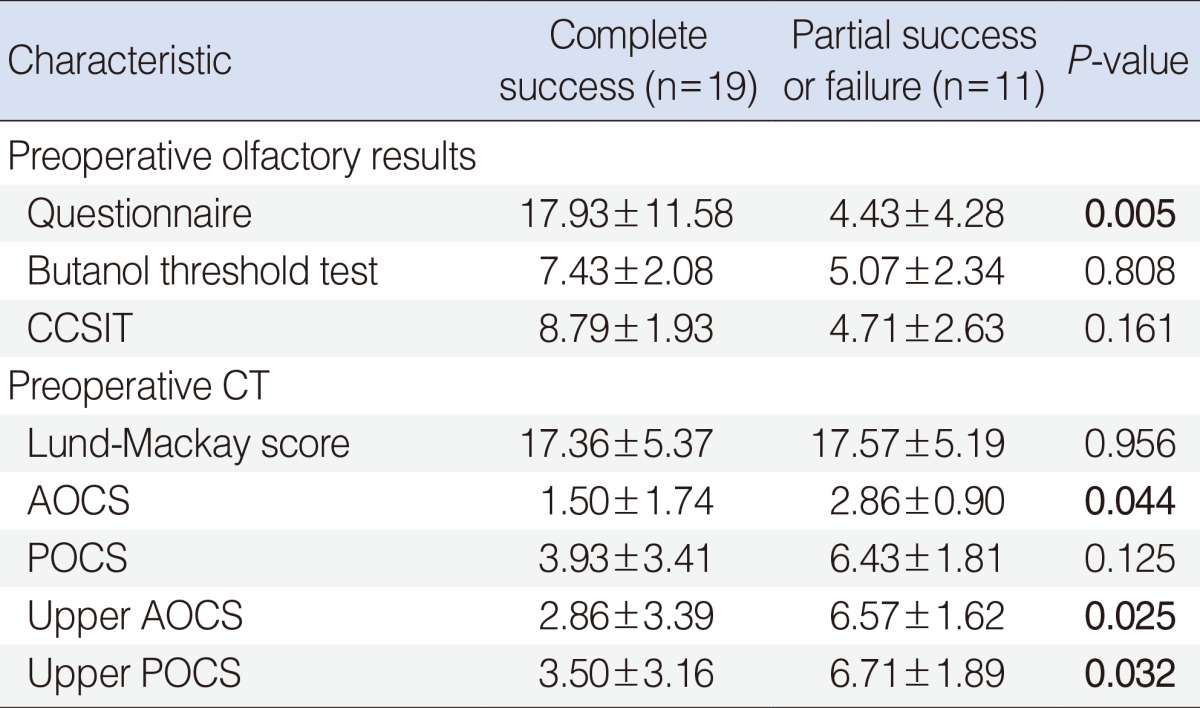
In the favorable wound healing group, patients with complete success had higher mean score of preoperative olfactory tests than those with partial success or failure. There was a significant difference in the preoperative questionnaire (Table 3) (P=0.005). In preoperative CT, Lund-Mackay score showed no differences between the two groups. However, there were significant differences in olfactory cleft scores, such as AOCS (P=0.044), upper AOCS (P=0.025), and upper POCS (P=0.032), between the two groups (Table 3).
DISCUSSION
Although CRS with NP has been proposed to cause more olfactory dysfunction than CRS [18], there have been few studies on postoperative olfactory changes in CRS with NP. One study has reported that the olfactory success rate defined as an improvement of threshold and identification tests, is 39% in CRS with NP [19]. An overall complete success rate of 48% in our study, having similar success criteria with a previous study, is higher than the earlier report. These results may be attributed to the study population with the small number of asthma patients and no revision cases, which are well-known prognostic factors for olfaction [19,20]. In addition, in our study, the favorable wound healing group had higher complete success rate of olfaction (63%) compared to the unfavorable wound healing group [25]. In the unfavorable wound healing group, characters such as discharge, edema, or recurrent polyps may block the olfactory cleft and may contribute to olfactory changes after ESS. To date, investigations of postoperative olfactory results have not considered the wound healing status; the widely variable results have been attributed to the different kinds of olfactory tests used, follow-up period, and study populations [4,7,8,18,21-23]. Our study implies that postoperative wound healing status may an important factor in the assessment of olfactory results after ESS.
In cases with favorable wound healing but no improvement of olfaction, the olfactory epithelium may be damaged in a partial or complete manner prior to surgery. Previous studies with olfactory mucosa biopsy specimens from patients with CRS suggest that inflammation of respiratory epithelium may contribute to reversible or irreversible damages of the olfactory epithelium [24,25]. In this context, we have previously documented that opacification of the olfactory cleft on preoperative CT may represent the possibility of irreversible damages of the olfactory epithelium and therefore, can be a predictor of olfactory changes after ESS [11]. Presently, opacification scoring of the upper olfactory cleft was additionally adopted on CT, because most olfactory epithelia are located in the upper part of the olfactory cleft. Patients with favorable wound healing but no improvement of olfaction were characterized by higher opacification in the upper part of the olfactory cleft, compared to those with improved olfaction. The collective data favor the suggestion that olfactory cleft opacification apparent on CT may be useful for giving prognostic consultation to ESS candidates in clinical practice.
Our data indicate a hierarchy of postoperative improvement of olfaction, from subjective to objective results and from threshold to identification. This pattern may be consistent with previous studies that reported threshold tests were improved much more than discrimination and identification tests after ESS [19,26]. Based on a consensus suggesting that receptors of like sensitivity are aggregated into particular regions of the mucosa, thus giving a different spatial representation for each odorant [27], partial irreversible injury of olfactory epithelium caused by mucosal inflammation might induce more discrimination disability than threshold impairment.
In conclusions, wound healing status is an apparent risk factor for postoperative olfactory improvement. In addition, preoperative opacification in the upper part of the olfactory cleft may predict bad olfactory results after surgery, even in patients with favorable wound healing.