INTRODUCTION
Hemangiomas are common lesions of the head and neck area, and they predominantly originate from the lips, tongue and buccal mucosa. Pathologically, it is debatable whether they are true neoplasm or vascular malformations. There are two main types of haemangiomas: cavernous and capillary. The capillary type is lobulated and it lacks a capsule, it is purplish in color and it infiltrates the involved glands. Microscopically, solid masses of cells and multiple anastomosing capillaries that replace the acinar structure of the gland are seen. The cavernous type is formed by dilated blood vessels or sinusoids lined by endothelium (1). Cavernous hemangioma of the external auditory canal (EAC) and tympanic membrane is rare, but this lesion is more common in the EAC. According to the previously reported cases (2-8), cavernous hemangioma seems to most frequently arise in the posterior portion of the EAC. However their incidence in the tympanic membrane is very rare and there have been only 4 such case reports in the literature according to a Medline search from 1970 to 2008 (9-12). We report here the 5th case of isolated cavernous hemangioma that was limited to the tympanic membrane and we review the relevant literature.
CASE REPORT
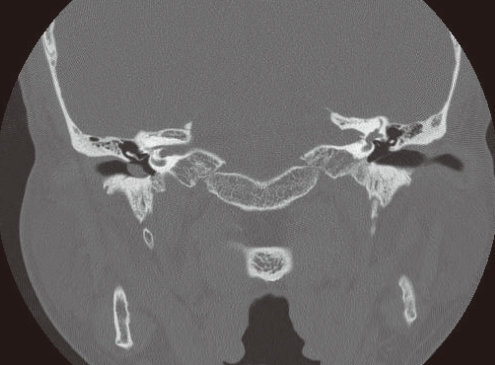
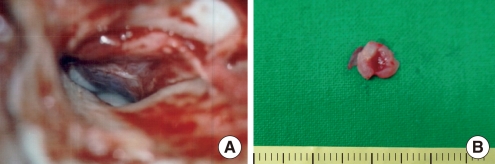
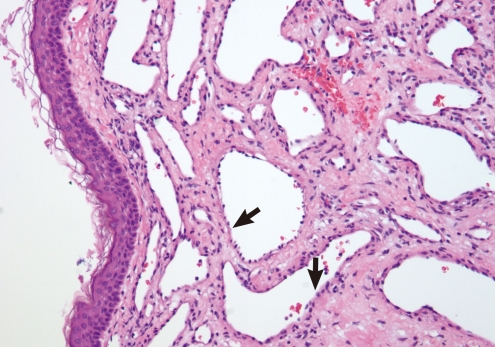
A 49-year-old man patient was referred to our department for evaluation of right-sided pulsatile tinnitus that he had experienced for the previous 2 years. The patient denied having hearing loss or vertigo and he had no evidence of facial palsy. His medical, surgical and family history was not noteworthy. Endoscopic examination of the EAC revealed a red-colored soft non-pulsatile mass that occupied part of the tympanic membrane (Fig. 1). The tympanic membrane was partially obscured by the mass and it was not clearly mobile. The endoscopic findings of the left ear were normal. A pure tone audiogram (PTA) showed high frequency mild sensorineural hearing loss in the right ear at 3,000-8,000 Hz (Fig. 2). Temporal bone computerized tomography (CT) showed an isolated soft tissue mass just lateral to the tympanic membrane. The size of the mass was 0.8├Ś0.5 cm. There was no evidence of bony erosion or middle ear invasion (Fig. 3). The patient underwent excision of the mass using the postauricular approach. A tympanomeatal flap was elevated to reveal a mass with involvement of the tympanic membrane. The mass was spongy on palpation, and it was removed en bloc with little bleeding. The size of the surgical specimen was 0.8├Ś0.5 cm (Fig. 4). The defect of the tympanic membrane was reconstructed by type I tympanoplasty and using a piece of fascia taken from the temporal muscle. Pathologic examination of the specimen showed a well-demarcated nodular lesion composed of dilated vascular spaces lined by a single layer of flat endothelial cells (Fig. 5). The preoperative pulsatile tinnitus disappeared immediately after operation. The postoperative hearing result was similar to the preoperative hearing result. The postoperative endoscopic examination showed an intact state of the neo-drum with good ventilation. There was no recurrence after 1 year of follow-up.
DISCUSSION
In 1983, Andrade et al. (10) reported the first case of cavernous hemangioma limited to the tympanic membrane in a 59-year-old man with a contralateral ear infection. According to the previously reported cases, cavernous hemangioma seems to most frequently arise in the posterior portion of the EAC. However the incidence of cavernous hemangioma limited to the tympanic membrane is very rare. They appear to arise from the lamina propria of the tympanic membrane.
Most of these patients are usually asymptomatic. Conductive hearing loss, tinnitus and aural fullness may be present. In the present case, pulsatile tinnitus was the chief complain and the tinnitus disappeared after surgical treatment. The endoscopic examination revealed a purple mass in the tympanic membrane. The differential diagnosis includes aural polyp, glomus tumor, arteriovenous malformation, granulation tissue and carcinoma of the EAC.
A temporal bone CT scan is the first choice for the evaluating the location and size of the lesion and middle ear involvement. The majority of the previously reported cases showed a normal middle ear. Only 1 case reported by Magliudo et al. (8) had cavernous hemangioma that initially involved the middle ear space through a small perforation in the tympanic memrane and the tumor had reached the handle and the short process of the malleus. For an advanced lesion, diagnostic angiography should be obtained to identify the blood supply to preoperatively assess the safety and feasibility of performing embolization (5).
Surgical treatment with en bloc excision is generally curative, and preoperative embolization is usually not necessary except for an advanced lesion. Recurrence of cavernous hemangioma because of inadequate excision has been reported (4). The endaural approach is generally used. In this case, we removed the mass by the postauricular approach due to the size of the mass. Subsequent reconstruction of the tympanic membrane is required. A large mass will require tympanoplasty with mastoidectomy (6).