INTRODUCTION
There is an increase in cochlear implant (CI) users due to expanding candidacy requirements, including prelinguistic deafness (1), more residual hearing (2), and bilateral CIs (3). Advancements in implant technology and speech-processing strategies have contributed immensely to the quality of life to the CI recipients, allowing them to have face-to-face and even over-the-phone conversations. However, individual patient outcomes still vary considerably. While some patients show vast improvements, such as speaking with unknown listener over the phone, other implant recipients unfortunately experience little benefit even after years of daily use of the device.
Much effort has been devoted to explore the sources of variability in cochlear implantation outcomes. Some studies have shown that patient-related factors such as duration of deafness, age at implantation, communication mode, types of educational setting, IQ, motivation, and family-related variables are correlated with speech perception performance (4-6). Others have shown dramatic improvements in CI recipients' speech recognition performance with advances in speech processing strategies (7) or by differences in CI recipients' initial listening experiences (8). Several researchers have also suggested that children and adults may benefit from intensive aural rehabilitation programs that include auditory training and strategies to enhance their understanding (9).
Auditory training is an intervention in which listeners are taught to make perceptual distinctions between sounds that are presented systematically (10). Programs may be formal or informal but are often structured around the type of training stimuli, the targeted skills, and the level of difficulty (11). An early study examining auditory training with CI users demonstrated significant enhancements of speech understanding in children but only a small improvement in adults (12). However, Fu et al. (13) later demonstrated that adults also improved significantly upon auditory training and that even CI users who completed a daily computerized training program benefited.
MATERIALS AND METHODS
Auditory training can be implemented either by a top-down or a bottom-up approach. The top-down approach, known as a synthetic training approach, aims to improve the efficiency of central processing (14); participants are trained to develop active listening strategies (e.g., attention to lexical or contextual cues). This approach targets higher levels of auditory processing and selectively uses lower-level auditory processing as needed. For example, the connected discourse tracking used by De Filippo and Scott (15) and Rosen et al. (16) reflects a top-down approach.
Analytic training is termed a bottom-up approach, because the intent is to improve the overall speech comprehension by focusing on the acoustic parts of speech messages. The reason is that if someone can reliably distinguish the acoustic elements of speech, then he or she should be better able to comprehend the larger units, such as sentences and paragraphs.
Efficiency of these approaches may illuminate the relative contribution of top-down and bottom-up auditory processing to speech understanding. For example, Gentner and Margoliash (17) found that both top-down and bottom-up processes modify the tuning properties of neurons during learning and give rise to 'plastic' recognition patterns for auditory objects.
Rather than invoking only one of the top-down or bottom-up processes, auditory processing most likely involves both mechanisms to some degree that may change according to the listening demands (18). Auditory training also include a series of exercises aimed at reaching a balance between achieving success on each successive task while maintaining the user's motivation level by increasing the difficulty. This training targets development of more sophisticated auditory skills over time.
Besides different training protocols, different training materimaterials may also influence training outcomes. A variety of speech materials have been used in previous studies (e.g., natural speech, synthetic speech, noisy speech, acoustically modified speech); these materials may include meaningful or nonsense speech. CI users with different disabilities may require different training materials.
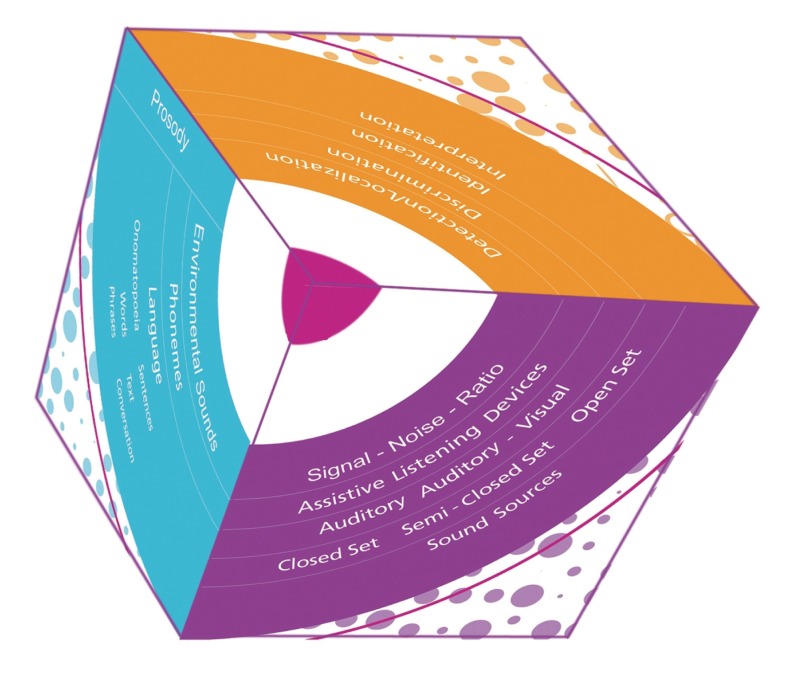
At KIDS Royal Institute for the Deaf in Belgium, an auditory training program called 'the Listening Cube' (19) was developed during the 20-year clinical practice with CI children and adults. All previously mentioned auditory training approaches and training materials can be included in this program. The Listening Cube (Fig. 1) is a three-dimensional auditory training model, based on the model developed by Corthals (20). It takes into consideration the sequence of auditory listening skills to be trained (dimension 1, the levels of perception); the variety of materials to be used (dimension 2, the practice material and prosody) and the range of listening environments (dimension 3, the practice conditions). It also alerts the therapists to increase their expectations and to allow improved perception of soft sounds and speech; improved speech understanding in background noise, as well as localization of sound and speech (21). While planning auditory training exercises, therapists can simply select combinations of items from these three different dimensions of the Listening Cube.
Levels of perception
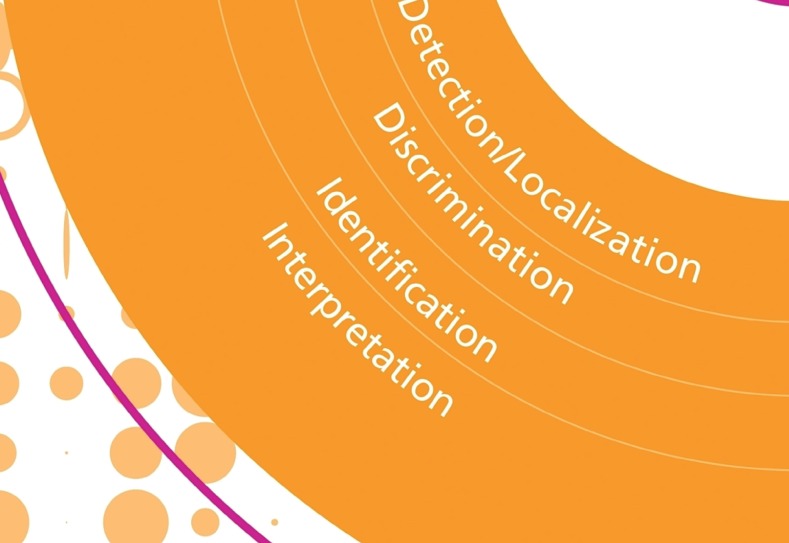
Hearing is viewed in terms of four different levels of perception in a hierarchy, which was already introduced by Erber (22) in 1982 (Fig. 2).
Detection is the most basic level of perception. It involves being able to notice and perceive the presence or absence of auditory stimuli and stimulates the exploration and discovery of the world of sound. Localization is the ability to detect the location of a sound source. This is an important topic in the case of bilateral stimulation. Discrimination is the perception of differences and similarities between sounds. Environmental sounds, phonemes, and words are all examples of different types of sounds which can be discriminated. In a discrimination task, the CI user must indicate if two or more items (such as /t/ and /k/ or /bi/ and /bo/) are the same or different. Identification of sounds is the ability to repeat or point to the stimuli heard. It involves the ability to match the perception of a sound to its actual source (or a picture of its source) and also to associate a speech sound (i.e., phonemes, words, phrases) with a larger context of language. Interpretation, also called processing or comprehension, is the ability to understand the meaning of auditory stimuli, not just to hear it. Understanding the content and meaning of a sound, phoneme, word, phrase, expression, sentence, or a larger utterance is central to interpretation. A good interpretation level stimulus, then, is one that requires the CI user to respond in a way to show that it was correctly processed or comprehended (e.g., following directions), giving a specific response, or summarizing something in his own words. These responses would indicate understanding that goes beyond just hearing.
Practice material
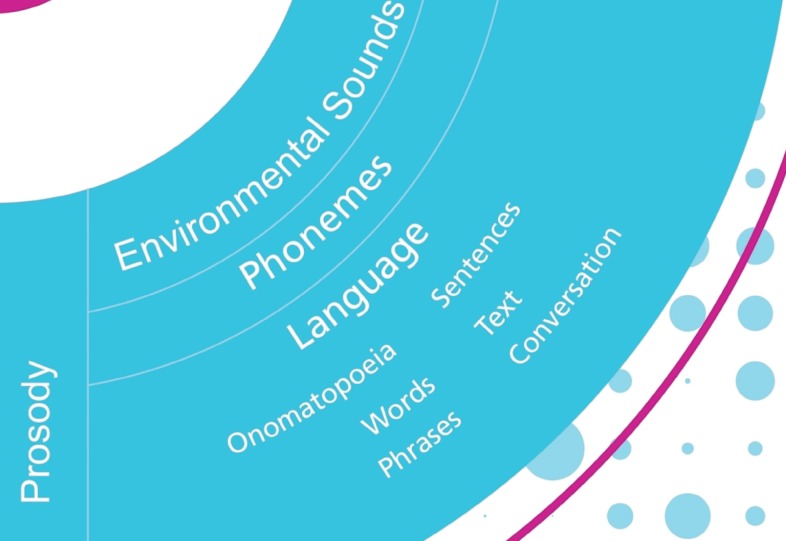
An overview of the practice material can be found in dimension 2 (Fig. 3). It consists of non-verbal (environmental sounds or phonemes in isolation) and verbal (speech) sounds. Language materials used for training are: onomatopoeia, phonemes, words, phrases, sentences, song and lyrics.
Prosody plays also an important role in the practice material. It refers to the rhythm, stress, and intonation in connected speech and includes suprasegmental (rhythm, duration, pause and pitch) and segmental (vowel, diphthong and consonant) characteristics.
Practice conditions
Auditory training should not only be conducted in ideal listening conditions (quiet environment, 1 M distance, or good speech intensity) but also under conditions that more closely resemble everyday-life situations that includes background noise, larger distances, and people who whisper. Fig. 4 shows an overview of the practice conditions of the Listening Cube.
Auditory training can be conducted while the person is wearing his/her own listening device, such as cochlear implant(s), or a cochlear implant and a conventional hearing aid, as well as by using assistive listening devices (ALDs) such as FM-systems, infrared systems or T-loops. In the case of CI users who are going to use these ALDs in daily life, it is especially important to practice using them during therapy to obtain assistance from the therapists for troubleshooting or adjustments.
Purely auditory signals, purely visual (speech reading), or a combination of both can be used for training. Speech reading adds the visual component (including eye contact and gestures) into the auditory training and makes the exercise much easier. It is also an option to start with visual support and to add on with increasing experience and confidence of the CI user.
In a closed-set activity, the person practices with a limited number of items (known by the person) via a set of objects, photos, drawings, or a list of written possibilities. In a semi-closed set activity, the person does not know exactly which items are being presented. Information is given about the stimuli to assist the person prior to the start of the exercise, for instance, by agreeing on a topic, theme, or a rule for the first few letters or phonemes of the possible responses. In an open-set activity, which is of the highest difficulty level, the person does not know the names of the items or anything about them beforehand. This would mean that there may be an unlimited number of possible responses.
The sound source can be the person, object, or animal that produces the sound. The possibilities for practice are almost unlimited: live voice (male, female, or children), back-ground noises, musical instruments, radio, TV, landline, mobile phone, CD, DVD, or an MP3. When designing sessions around the practice material and around the person's needs, difficulty level should always be kept in mind, listed here from easiest to most difficult:
From closed to open-set
With and without speech reading
Without and with background noise
From a short distance to a longer distance
From easy to difficult practice material (from large to small auditory differences, from short to long utterances, from easy to difficult language level)
All combinations of three dimensions
Auditory training always starts with large contrasts. These are large differences in sound characteristics, which are more easily perceivable and the degree of difficulty becomes bigger by reducing the contrasts.
RESULTS
Although CI-users were previously shown to benefit from intensive aural rehabilitation programs that include auditory training and strategies to enhance their understanding of the incoming speech signal (9), there is currently no consensus concerning the optimal rehabilitation program or technique (23).
The Listening Cube is a rehabilitation program developed in clinical practice which allows integration of several rehabilitation techniques. Due to the many variables that influence the outcome, it is difficult to make strong statements about the results. However, we can report that this auditory training model is very successful, as described by more than 250 therapists in Belgium and the Netherlands. Most of them chose to use the Listening Cube in their daily practice with children and adults with a hearing loss, especially in those wearing cochlear implants.
DISCUSSION
Many challenges remain in designing effective aural rehabilitation programs for CI users. It is important to develop training protocols and materials that will provide rapid improvements over a relatively short time period and to determine that the training apply to the many listening environments that CI users encounter in the real world. It is also important to ensure the effectiveness of the training programs, while minimizing the time commitment required of the CI user and maximizing training outcomes.
The Listening Cube is a tool for planning therapeutic sessions which are both challenging and appropriate for CI users' individual needs. The three dimensions of the cube - levels of perception, practice material, and practice conditions - can serve as a visual reminder of the task analysis and other considerations that play a role in structuring therapy sessions.
This training model is very successful in Belgium and the Netherlands since the first publication in the Dutch language in 2003. Because of the large demand by professionals in the field of rehabilitation of people with a hearing loss, we began to conduct training courses twice a year. Most professionals attending these courses decided to implement it in the rehabilitation of children and adults with a hearing loss, especially in those wearing a cochlear implant. In 2008 the Austrian CI-company MED-EL decided to implement the Listening Cube into their rehabilitation programs and to translate it from Dutch to English, French, German and Spanish (24). Since then, the Listening Cube is used for rehabilitation of CI-users all over the world.