INTRODUCTION
Carcinosarcoma (also known as pseudosarcoma, pseudosarcomatous squamous cell carcinoma, pleomorphic carcinoma, and spindle cell carcinoma) is a highly malignant tumor characterized by dual malignant histologic differentiation of the epithelial component consisting of a focally squamous cell carcinoma and a mesenchymal component having a sarcomatoid stroma [1,2].
Carcinosarcoma may arise in any squamous epithelium of the body, however its occurrence is extremely rare in the sinonasal cavity [3-13].
We present a case of a carcinosarcoma located in the maxillary sinus that was is aggressive and displayed a high recurrence rate even when a multimodality therapeutic approach was adopted.
CASE REPORT
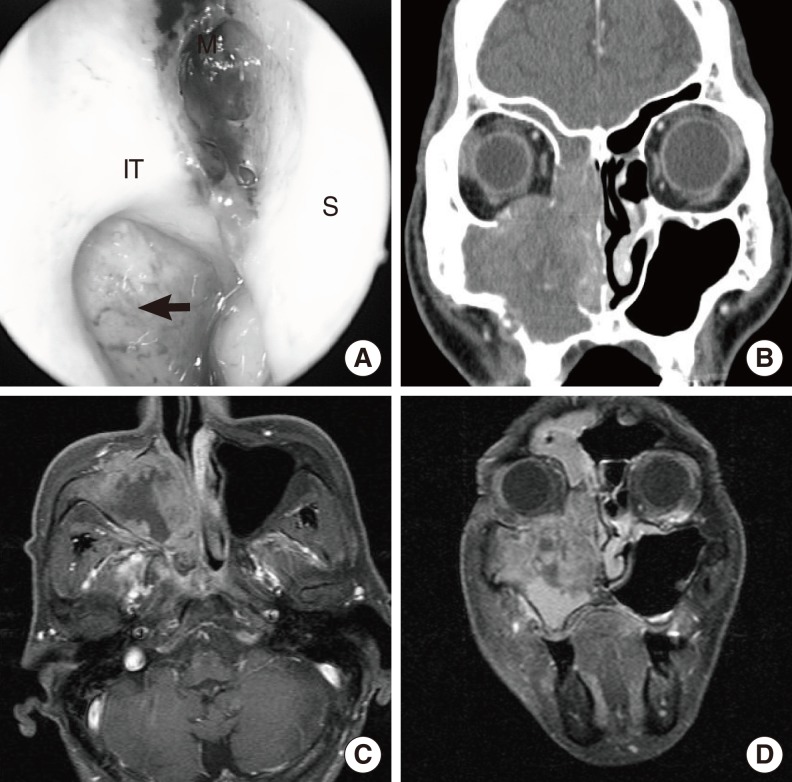
A 62-year-old male was admitted to the emergency room due to uncontrolled epistaxis and complaining of swelling and tenderness in the right cheek. The patient was receiving warfarin as an anticoagulative measure, having previously suffered a stroke. An examination of the nasal cavity was not possible at the emergency room due to the severity of bleeding. Nasal packing was applied to staunch the bleeding. Two days later, when the nasal packing was removed and endoscopic examination performed, a mass in the middle meatus and bulging of the medial wall of the maxillary sinus were observed (Fig. 1A). Computed tomography (CT) and magnetic resonance imaging (MRI) scans revealed a large mass comprised of soft tissue with an ill-defined outline and an irregular peripheral enhancement on the right maxillary sinus. The mass had pushed against the right inferior wall of the maxillary sinus; destroyed the infraorbital foramen; completely destroyed the medial wall of the maxillary sinus; partially damaged the superior, middle and inferior turbinate; and obstructed the entire right nasal cavity. The lateral, anterior, and inferior walls of the right maxillary sinus were focally destroyed and a focal tumor extension was exposed. The mass extended superiorly to some part of the ethmoid sinus but did not involve the sphenoid sinus and frontal sinus (Fig. 1B-D).
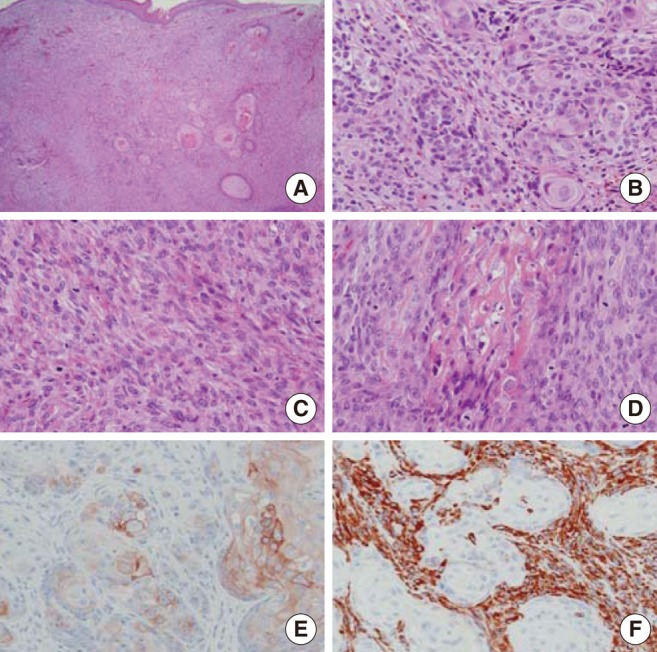
An endoscopic biopsy revealed a carcinosarcoma with an osteosarcomatous element by Hematoxylin-eosin staining and immunohistochemical stain (Fig. 2). Fluorodeoxyglucose positron emission tomography (FDG PET)-CT was used to evaluate metastasis to adjacent organs. FDG PET-CT revealed the presence of large mass of soft tissues with increased FDG uptake accompanied by bony erosion in the right maxillary sinus. Also, nodular lung lesions with increased FDG uptake in lateral basal and posterior basal segment of right lower lung were observed. CT-guided lung biopsy for metastasis evaluation indicated only chronic inflammation. Hence, the clinical TNM staging of this patient was T3N0M0 (stage III).
A surgical resection with postoperative chemoradiation therapy was planned and the patient underwent a total maxillectomy on the right side. Examination in the operating room revealed a large tumor filling the nasal cavity, maxillary sinus, and ethmoid sinus. The tumor had eroded through the inferior and medial orbital walls, however, periorbital invasion was not evident. The tumor had also eroded the lateral bony wall of the maxillary sinus. After the surgical resection, frozen biopsies of all margins were grossly clear.
The patient's postoperative course was uncomplicated, and he received postoperative radiation therapy with a total dose of 5,580 cGy. However, during the radiation therapy, a mass lesion in the periorbital area was found in an endoscopic examination. The pathology was indicative of carcinosarcoma. As a consequence, wide local excision was performed on the mass and the patient received a full course of irradiation, followed by chemotherapy (Cisplatin+5 fluorouracil+Taxotere). Two months later, the patient developed a massive recurrence infiltrating the orbit, cheek, and the masseter muscle. The patient decided not to receive further surgical treatment or chemotherapy, and was lost to follow-up.
DISCUSSION
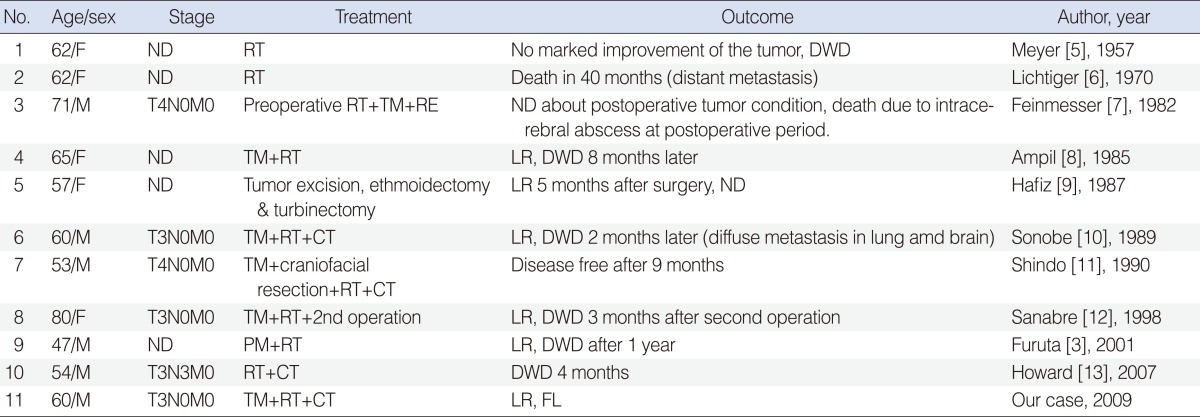
Carcinosarcoma is a biphasic tumor composed of dual components: an epithelial portion with squamous cell carcinoma and sarcomatoid lesion. This tumor can arise in any squamous epithelium of the body, such as the respiratory tract, upper aerodigestive tract, and reproductive organs. In the head and neck region, it is most commonly found in the pharynx or larynx [2]. This tumor is extremely rare in the sinonasal cavity, as indicated by the few case reports available (Table 1) [3,5-13].
Because of this rarity, tumor histogenesis, clinical course and resulting prognosis, and management are contentious issues.
Concerning histogenesis, whether the cellular composition of carcinosarcoma is that of a true heterologeous tumor or whether it originates from a single malignant component having both epithelial and mesenchymal differentiation [3] is debatable. Recent electron microscopic and immunohistochemical investigations revealed epithelial differentiation in some of the spindle cells in the sarcomatous element, suggesting that the sarcomatous element is derived from mesenchymal transformation of the carcinoma cells [6,14].
From the known cases (Table 1), carcinosarcoma of the maxillary sinus seems to preferentially appear in older patients. Clinically, the symptoms are often nonspecific, but unilateral nasal obstruction and bleeding are initial symptoms. Because of the high stage presentation at the time of diagnosis, this tumor presents significant therapeutic challenges and a fateful prognosis for the patient.
The management for this rare disease still remains undetermined. Prognosis has been better in patients treated with surgery and adjuvant radiation therapy. Radiotherapy might be administered for postsurgical palliation of local recurrence. Carcinosarcoma in the maxillary sinus was treated by surgery in eight of the 11 cases (Table 1). Except for one case, radiotherapy was used for the treatment of the tumor. But, clinical effectiveness of chemotherapy is impossible to determine with statistical significance due to the small number of cases to date. Although an accurate estimation of survival outcome is not conclusive, carcinosarcoma at the maxillary sinus confers a poor survival rate and a high local recurrence rate. In the known cases, tumors in the maxillary sinus recurred after management in seven of 11 cases (Table 1). Local recurrences and metastases typically were lethal. An overall mortality rate of 42% at 30 months was reported in carcinosarcoma at other sites [4]. Survival periods were from 2-40 months and local recurrences eventually occurred in most cases (Table 1).
When a carcinosarcoma tumor is located within the maxillary sinus, multimodal therapy (i.e., surgery, radiotherapy, and/or chemotherapy) should be considered. Also, before aggressive multimodal therapy is initiated, patients should be counseled concerning the tendency for aggressive patient behavior, poor prognosis, and likelihood of recurrence.