INTRODUCTION
Congenital cystic lesions of the oral cavity are very rare [1]. The differential diagnosis of intraoral cystic lesions include: ranula, lymphatic malformation, dermoid cyst, epidermoid cyst, teratoma, heterotopic gastrointestinal cyst and duplication foregut cysts [1]. Histologically, all dermoids are lined by epidermis [2,3]. The contents of the cyst lining determine the histological category of the cyst: epidermoid, if epidermis is lining the cyst; dermoid, if skin adnexa are present; or teratoid, if other tissues such as muscle, cartilage, and bone are present [2,3].
Epidermoid cysts are benign developmental anomalies [1]. They can develop anywhere in the body, with an incidence ranging from 1.6 to 6.9% occurring in the head and neck area and 1.6% within the oral cavity [1]. They represent less than 0.01% of all oral cavity cysts [1]. An epidermoid cyst presents as a slow-growing asymptomatic mass; they are usually diagnosed only after they have reached a considerable size [1,2,4]. Even if they are congenital, the diagnosis is usually possible during the second or third decade of life [1,4]. Therefore, these cysts are uncommon in neonates. However, if they are present and not recognized and treated expeditiously, these anomalies may obstruct the upper airway and gastrointestinal tract and potentially can be fatal [1,3].
Here we report a case with a congenital epidermoid cyst of the oral cavity diagnosed prenatally by sonography and discuss the importance of perinatal management with the coordination of neonatologists, obstetricians, pediatric and oral-maxillofacial surgeons.
CASE REPORT
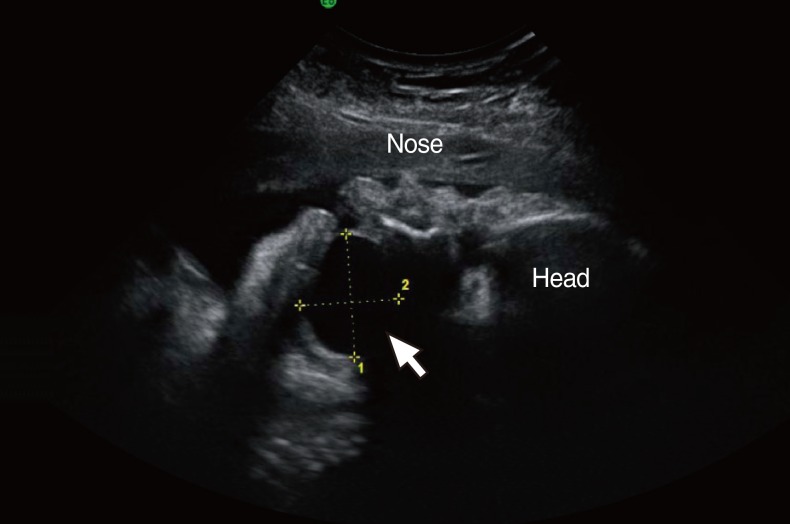
An intraoral cyst in a fetus was detected by prenatal sonography at 38 weeks of gestation. This was the first pregnancy of a 32-year old woman with no previous medical problems. The mother was referred to our obstetrics department where ultrasound scanning confirmed the presence of a large cystic mass, measuring 30├Ś25 mm in the oral cavity (Fig. 1). Because of regular labor pains, the mother underwent emergency cesarean section delivery at 38 weeks and 3 days, with a multidisciplinary surgical team including pediatric and oral-maxillofacial surgeons. Supplies and equipment for an emergency tracheostomy were made available prior to the delivery in case respiratory distress occurred and intubation was not possible. However, the infant did not require intervention to secure the airway. A 2,918 g female infant was delivered and transferred to the Neonatal Intensive Care Unit.
On examination the infant did not present with dyspnea or dysphonia. Clinical examination showed normal facial features and there was no extra-oral swelling or lymphadenopathy. Intraorally, there was a 20├Ś20 mm sublingual mass displacing the tongue laterally. The swelling was a tense, non ulcerated, smoothsurfaced, well-defined cystic lesion located in the right sublingual region (Fig. 2). The lesion was slightly movable, and rubbery. No additional mucosal lesions were present.
The postnatal computed tomography (CT) scan of the neck confirmed the presence of a 30├Ś22 mm well circumscribed non-enhancing cystic mass in the right sublingual region (Fig. 3). A neck sonography revealed a cystic lesion without separation or a solid portion in its inner side. Two days later, under general anesthesia and with intraoral tracheal intubation, the patient underwent surgical removal of the mass. The cyst was dissected from the surrounding tissues and removed. The wound was closed primarily. Macroscopically, the lesion appeared encapsulated. The histopathological sections showed a cyst lined by mature keratinized squamous epithelium. The final histological diagnosis was an epidermoid cyst.
Postoperatively, the infant was extubated after surgery in the operating room. The airway and respiratory management needs to be closely monitored. No airway difficulty was experienced in the postoperative period. Oral feeding was started on the next postoperative day. The infant made a good recovery and by three days postoperatively, managed full feeding orally. The patient was discharged three days later. At follow-up six months later, tongue movements were normal, and feeding remained unimpaired. And then the patient continues to do well with no evidence of recurrence.
DISCUSSION
The widespread use of prenatal sonography can lead to earlier diagnosis and allows for appropriate counseling and preparation for delivery. Cystic oral lesions detected by prenatal sonography include many different diagnose. These include: ranula, lymphatic malformation, dermoid cyst, epidermoid cyst, teratoma, heterotopic gastrointestinal cyst and a duplication foregut cyst [1,4]. The prenatal diagnosis of ranulas, mucoceles, lymphatic malformations and enteric duplication cysts has been reported in many cases.
Epidermoid cysts are extremely rare in infancy [1]; no more than 30 cases of congenital cysts of the oral floor have been reported. Because they are slow-growing masses and usually diagnosed only after they have reached a considerable size [1,2,4]. In one case, a newborn was reported, but she presented to the hospital with symptoms of feeding difficulty and tachypnea [4]. In some cases, the prenatal diagnosis of a teratoma has been previously reported. However, there is no prior case of the prenatal diagnosis of an epidermoid cyst to date.
Large intraoral cysts in the developing fetus or newborn infant may cause airway obstruction [1,3]. This can cause respiratory compromise at delivery with difficulty in establishing an airway resulting in extreme hypoxemia and death [1,4]; when clinicians are not prepared there is an increased risk for significant morbidity. In our case, we attended with a multidisciplinary surgical team including pediatric and oral-maxillofacial surgeons.
The preoperative evaluation of lingual cystic masses in newborns includes palpation, high-resolution sonography, CT or magnetic resonance imaging (MRI) [2,4]. High-resolution sonography has been found to be very useful in revealing the nature of the mass and in delineating its extension [1]. CT and MRI allow more precise localization of the lesion however, they have risk of sedation [1,5]. Epidermoid cyst is typically revealed by CT as a well-defined, lobulated mass with hypoattenuation similar to that of fluid. MR imaging of an epidermoid cyst typically depicts a cystic mass, hypointense on T1-weighted images and hyperintense on T2-seighted images [5].
Surgical enucleation is the only effective treatment. The prognosis is very good, with a very low incidence of relapse [1,3,4]. Surgical excision is normally achieved without major complications.
This case illustrates the value of accurate prenatal diagnosis and carefully planned perinatal management using a team approach with neonatologists, obstetricians, pediatric and oral-maxillofacial surgeons.
In conclusion, identification of epidermoid cysts in the oral cavity is uncommon in neonates [1]. If not recognized and treated expeditiously these anomalies may obstruct the upper airway and gastrointestinal tract and potentially can be fatal.