INTRODUCTION
Although benign soft-tissue tumors represent 2%-5% of all salivary gland neoplasms [1], lipoma rarely occurs in the salivary glands, accounting for less than 0.5% of all parotid gland tumors. Lipomas are classified as simple lipoma, fibrolipoma, angiolipoma, spindle cell lipoma, and pleomorphic lipoma. Sialolipoma, a newly reported variant of salivary gland lipoma, is a well-circumscribed salivary gland tumor composed of mature adipocytes and glandular tissue. Since the first seven cases were reported in 2001 by Nagao et al. [2], 23 additional cases of sialolipoma have been reported to date [3]. We report a case of oncocytic sialolipoma, a new pathological subtype of sialolipoma described by Pusiol et al. [4]. This case is only the second reported case of oncocytic sialolipoma and the fourth case of submandibular gland sialolipoma.
CASE REPORT
A previous healthy 43-year-old woman was seen for evaluation of swelling in the right submandibular region. The patient first noticed the mass 2 months before visiting the hospital. She had no pain, trismus, or discomfort during eating, but complained of cosmetic problems. The mass was very soft and movable within the submandibular region; no tenderness was reported during physical examination.
Ultrasonography (USG) showed that the mass was of a relatively heterogeneous, hypoechoic nature, with ill-defined margins compared to typical submandibular glands. The tumor was located in the superficial and deep portions of the normal submandibular gland and extended externally to the gland (Fig. 1A). A computerized tomography (CT) image revealed a fatty mass with an irregular margin. Multiple soft tissue density was seen inside the mass in the right parapharyngeal space and submandibular region (Fig. 1B). Because the mass was located at the superior and medial aspect of the submandibular gland, the residual gland was displaced inferolaterally, creating the cosmetic problem about which the patient complained. As we had no previous experience with sialolipoma, our clinical impression of the mass was that it was a simple lipoma of the submandibular gland.
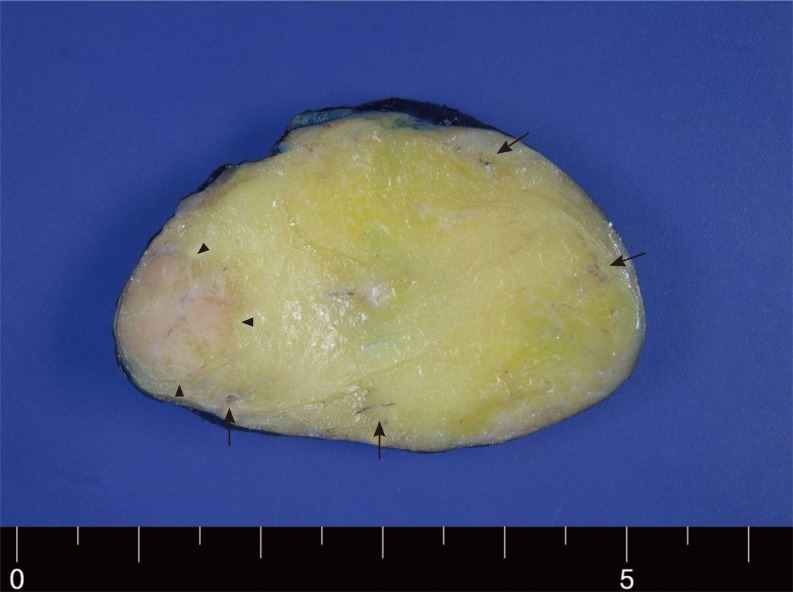
Tumorectomy with preservation of submandibular gland was performed under general anesthesia via submandibular incision. A marginal mandibular branch of the facial nerve was identified and preserved. Because the tumor was well-encapsulated, it could be easily dissected from the main submadibular gland. The tumor measured 4 cm in its largest dimension and had a fatty consistency like a simple lipoma. Gross examination revealed that the tumor was well-circumscribed, soft, yellowish, and had a well-demarcated light pink-colored nodular component surrounded by fatty tissue. Ill-defined brown lesions were scattered around the nodule; histological examination identified these as an oncocytic nodule and glandular tissue (Fig. 2).
Microscopic examination showed that the tumor was encapsulated by a thin fibrous capsule; the majority of the tumor consisted of adipocytes, which had no histological differences from simple lipoma. Salivary gland tissues within the tumor were sparse. Those present were surrounded by adipocytes; hence, theses gland tissues were completely isolated from the tumor capsule. An oncocytic nodule was found surrounded by adipose tissue and mainly located at the periphery of the tumor, adjacent to ductal structures (Fig. 3A). The nodule, measuring about 1 cm across, was composed of large round to polygonal cells with fine granular, eosinophilic cytoplasm, and round vesicular nuclei with occasional nucleoli (Fig. 3B).
DISCUSSION
Lipomatous tumors admixed with salivary gland tissue have been studied with interest for the last decade. New tumor types, including sialolipoma, lipoadenoma, oncocytic lipoadenoma and oncocytic lipoadenoma with sebaceous differentiation have been described [4]. Oncocytic sialolipoma of the salivary gland is a unique benign tumor that has recently been described in the literature, but is not currently included in the World Health Organization classification of salivary gland tumors. Since the first report of 7 cases of sialolipoma by Nagao et al. [2], a total of 30 cases of sialolipoma have been reported [3]. These accounted for 0.3% of salivary gland tumors. The incidence of oncocytic sialolipoma could not be determined from the data due to the rareness of this tumor [3,4].
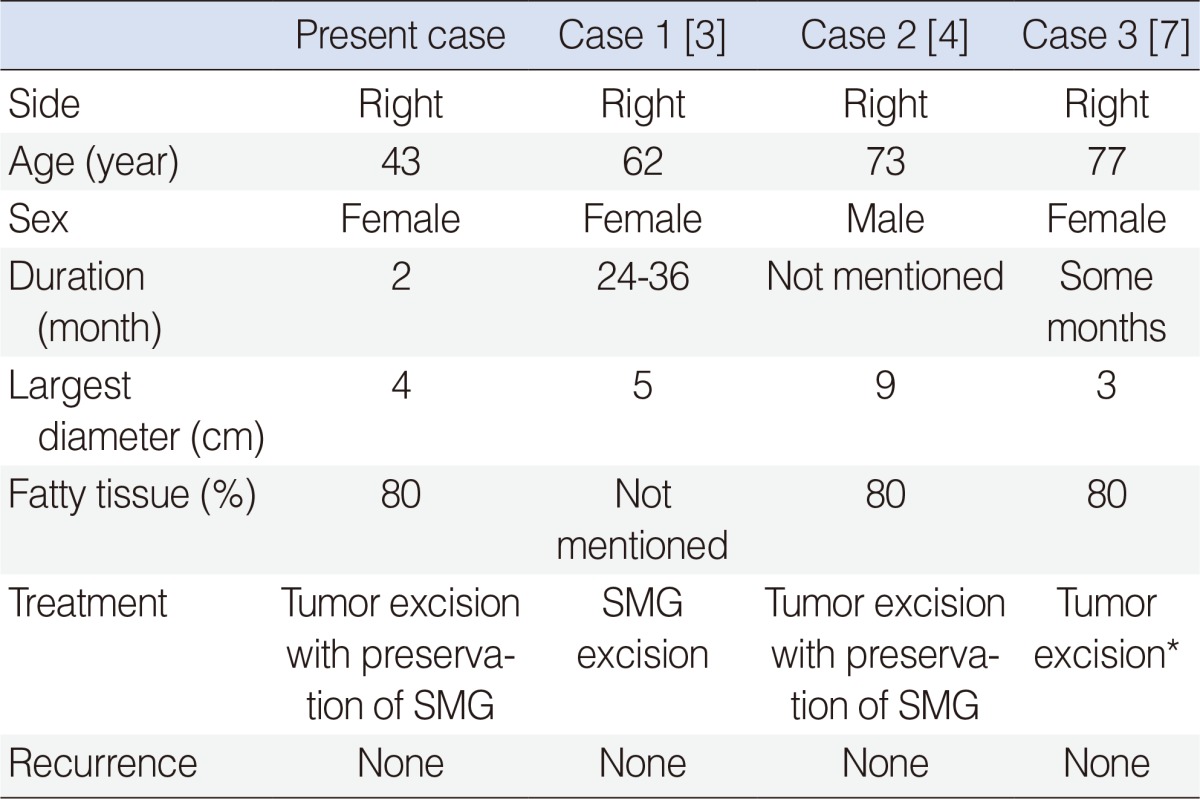
Sialolipoma is characterized as a well-circumscribed, encapsulated mass, composed of benign, neoplastic, adipose tissue with scattered glandular components [2]. Ductal cells of glandular components may show ectasia with fibrosis and focal oncocytic metaplasia. The histogenesis of the various components is unclear, but previous studies presumed that the glandular components of sialolipoma have become entrapped during lipomatous proliferation, rather than representing simple neoplastic elements [2,4]. Adipose tissue composes a higher percentage of parotid gland sialolipomas (90% or more) than sialolipoma arising in other sites (50%-80%) [2,5,6]. Four cases of sialolipomas arising in the submandibualr gland were analyzed and found to have a proportion of adipose tissue as high as that of the parotid gland sialolipomas [3,4,7] (Table 1). Hence, a more accurate statement might be that major salivary gland sialolipomas have a higher proportion of adipose tissue than do those of the minor salivary glands.
According to a review of 28 cases of sialolipoma by Jang et al. [3], the most common site for sialolipoma was the parotid gland (17 cases), followed by the palate (4 cases); sialolipoma arising from the submandibular gland was found in only 2 cases. The age distribution of patients ranged from 7 weeks to 84 years; 1 case reported by Hornigold et al. [8] was congenital in onset. Previous studies had reported that sialolipoma predominantly affected males [2,5], but this review found the male to female ratio to be 1:1. The mean tumor size was about 3.5 cm, with a range of 1-7cm; 7 tumors were over 4 cm. Interestingly, all 4 cases of sialolipoma of the submandibular gland were on right side; 3 of the 4 tumors were in females, and the mean tumor size was 5.2 cm.
CT and USG are helpful for preoperative diagnosis of conventional lipomas. Their high fat content typically causes low attenuation in CT [6]. Lipomas may present as heterogeneous hypoechoic lesions in USG, with echogenicity similar to that of subcutaneous fat tissue. However, imaging studies do not distinguish sialolipoma from conventional lipoma. Although fine needle aspiration cytology may be useful for diagnosis of lipomatous tumors of the salivary gland, the definitive diagnosis of sialolipoma is based on histopathologic features [6]. As a rare tumor, oncocytic sialolipoma of the salivary gland can have differential diagnoses, primarily other tumors with a large adipose tissue component.
Sialolipoma is a proliferation of mature adipose tissue, surrounded by a thin fibrous capsule. It is characterized by islands of epithelial salivary glandular components that consist of ductal, acinar, basal, and myoepithelial cells that are enclosed in mature adipose tissue [2]. Lipoadenoma is characterized by an admixture of mature adipose tissue and branching epithelial tubules that lack myoepithelial cells. Immunohistochemical examination reveals no acini [1,4]. The presence of a fibrous capsule can easily distinguish sialolipoma from lipomatosis; the presence of normal salivary gland with duct dialatation and fibrosis precludes the possibility of a pleomorphic adenoma with extensive adipose content [2,9]. If a tumor has oncocytic nodules as in our case, it should be differentiated from oncocytoma, which has some malignant potential. Distinguishing between these 2 tumor types is not difficult because oncocytic nodules of sialolipoma are surrounded by abundant adipocytes adjacent to normal glandular structures.
To our knowledge, 5 cases of oncocytic lipoadenomas have been previously reported in the literature [1]. Our case in only the second report of oncocytic sialolipoma. In the first report, oncocytic sialolipoma was characterized as sialolipoma with oncocytic adenoma in the tumor. The oncocytic micronodules have been considered to be the result of oncocytic metaplasia and hyperplasia of ducts. In our case, an oncocytic micronodule was found adjacent to ductal structures and isolated from fatty tissue, just as reported by Pusiol et al. [4]. This arrangement suggests that the oncocytic nodule originated from ductal cells, which became separated from the ducts by proliferation of adipose tissue [4].
Treatment for sialolipoma is complete surgical excision of the tumor. Because the tumor in our case was well-encapsulated and the initial impression was that of a simple lipoma, the treatment of choice was tumorectomy with preservation of the submandibular gland. Superficial parotidectomy has been performed in most cases of parotid gland sialolipomas. No recurrences have been reported in any of the 30 cases of sialolipoma [3,5,6].
In conclusion, sialolipoma is a very rare, but distinct salivary gland neoplasm. It is found predominantly in parotid glands, but could develop in any salivary gland. Many variations of sialolipoma such as oncocytic change and sebaceous differentiation are possible. As a newly described tumor type, care should be taken to distinguish from other salivary gland neoplasms such as simple lipoma, pleomorphic adenoma, or oncocytoma.