To the editor:
We read with interest the article by Cho et al. [1] published in Clinical and Experimental Otorhinolaryngology where the authors were the first to report a patient who showed fluctuating mixed hearing loss as one of the initial manifestations of IgG4-related disease (IgG4-RD). This patient was a 66-year-old woman with IgG4-RD present with fluctuating mixed hearing loss and middle ear effusion. The serum IgG4 level was elevated and pathological examination revealed dense infiltration of IgG4-positive lymphocyte in the renal parenchyma, lung tissue and lacrimal glands. Treatment with intravenous methylprednisolone at a dose of 60 mg daily resulted in improvement of hearing loss.
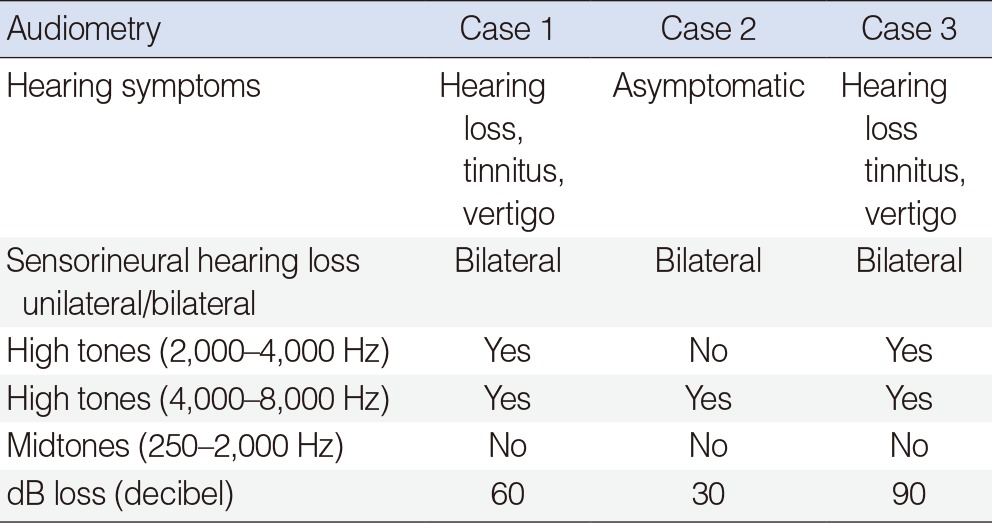
We describe three cases of sensorineural hearing loss (SNHL) due to IgG4-RD (Table 1) (Umehara's comprehensive criteria 2011 [2]), two men and a woman with ages between 35 and 75 years and a follow-up time of 5 to 12 months. Two patients showed symptomatic hearing loss and tinnitus and one had a history of vertigo. In all of them, audiometric studies disclosed bilateral and symmetric SNHL at high frequencies between 30 db and 90 db (Table 2). Unlike the report by Cho et al. [1], we did not see mixed conductive alterations. Improvement of hearing loss was observed with meprednisone 60 mg/day and metotrexate 15 mg/week.
Autoimmune SNHL is a rare disease of unknown etiology first described McCabe [3] in 1979. It has been reported as an otological manifestation of Wegener granulomatosis, polyarteritis nodosa, systemic lupus erythematosus (SLE), rheumatoid arthritis, antiphospholipid syndrome, Sj├Čgren syndrome, Cogan syndrome, giant-cell arteritis, ulcerative colitis, ankylosing spondylitis, and Crohn disease.
In 2006, we reported a prospective and descriptive study showing that 20 of 30 patients with SLE (66%) revealed an asymptomatic SNHL at high frequencies, bilateral and symmetric with statistically significant differences when compared with a control group. Vasculitis, microinfarction of the capillaries or arterioles, and thrombosis in the otologic region were postulated as the causes of SNHL [4].
The 3 cases with IgG4-RD presented bilateral and symmetric SNHL as SLE patients but they differ from the case reported by Cho et al. [1] in that they did not show fluctuating mixed hearing loss as initial manifestation of IgG4-RD. Patient one and three also had SNHL as initial manifestation and IgG4-RD was confirmed in the three cases by histological and immunopathologic examinations (Umehara's comprehensive criteria 2011). They all had good responses to treatment with glucocorticoid.
An autoimmune mechanism is assumed in patients with bilateral progressive or fluctuating mixed hearing loss, especially when they respond to immunosuppressive treatment. It suggests that the inner ear can be the target of this systemic autoimmune disease resulting in otitis media and also affecting the respiratory epithelium, including the one in the middle ear mucosa. Because vestibular dysfunction may progress slowly, the patient's dizziness may not be of a whirling nature or associated with a definite history of vertigo or imbalance [1].
IgG4-RD is known to involve various organs and can be diagnosed by elevated serum IgG4 level and infiltration of IgG4 positive cells in those organs. At the International Symposium on IgG4-RD, where the consensus document on nomenclature was drafted, the attendees agreed that a minimum of 5 reports of involvement in any given organ should be published before such organ could be included as an individual manifestation of IgG4-RD [5].