INTRODUCTION
Foreign body aspiration into the airway is an important and common accident in pediatric patients and adults with a compromised laryngeal function [1,2,3,4,5]. Because the retained foreign bodies can result in many pulmonary complications, early diagnosis and intervention is very important in managing these patients [6,7,8,9].
Bronchoscopy, particularly rigid bronchoscopy, is a key procedure for diagnosis and retrieval of a foreign body [10,11,12]. Conventionally, this technique involves the insertion of a rigid bronchoscope and naked eye manipulation. With the advancement of medical imaging and endoscope systems, the incorporation of an endoscope to the rigid bronchoscopy procedure has greatly improved the accuracy of diagnosis and manipulation with less morbidity [13,14]. Furthermore, combining optical forceps with endoscopy has enhanced one-hand manipulation under endoscopic guidance [14].
Currently available optical forceps range from 2.9 to 5.5 mm in diameter. Among them, a 2.9 mm sized optical forceps (d=2.9 mm, length 30 cm; Optical Pediatric Forceps 10020ATA Straight Forward Telescope; Stortz, Tuttlingen, Germany) is very useful for very young age (<3 years of age) pediatric patients, who usually require a 3.0 to 4.5 mm sized rigid bronchoscope. Larger optical forceps, endoscopes, and forceps are too big to be inserted in these patients, and the clinical advantage of an endoscope-guided manipulation during rigid bronchoscopy procedure is rarely achieved in very young age patients, except using 2.9 mm optical forceps.
We present here a method of endoscope-guided rigid bronchoscopy technique in very young age patients, even without 2.9 mm optical forceps, and refine each step of the rigid bronchoscopy procedure. The clinical benefits of this approach were confirmed by comparison of the outcomes between the bimanual endoscope-assisted techniques and the conventional method. We believe this article will help patient care as well as learning, education and documentation of the rigid bronchoscopy technique.
MATERIALS AND METHODS
Bimanual endoscope-assisted rigid bronchoscopy: instruments and techniques
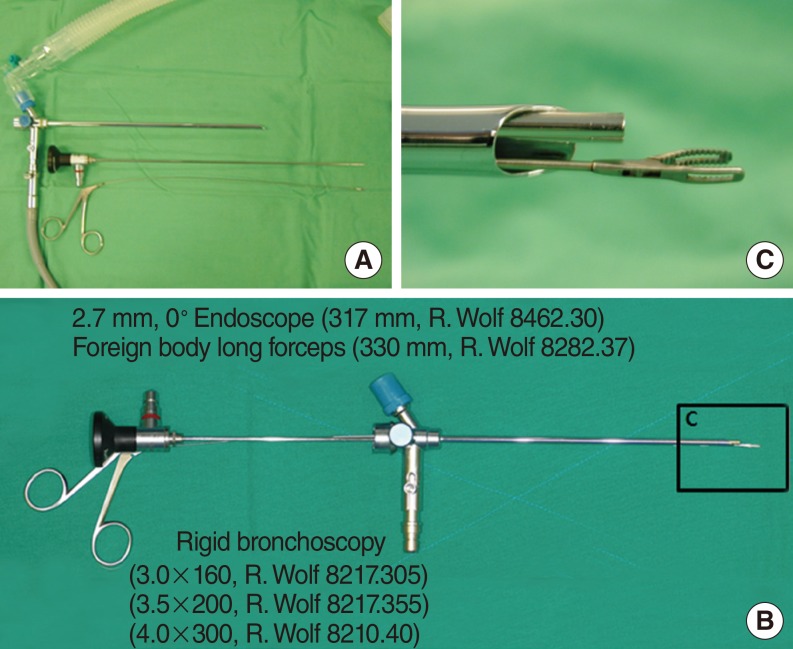
Bimanual endoscope-assisted rigid bronchoscopy techniques comprises five consecutive procedures: (1) endoscope-guided approach, (2) rigid bronchoscope positioning in situ by an assistant, (3) dis-impaction and mobilization of the impacted foreign body, (4) endoscope-guided retrieval, and (5) second-look procedure (Video clip 1, Supplementary material). The equipment for the procedure were 2.7 mm, 0° straight endoscope (317 mm, R. Wolf 8462.30, Vernon Hills, IL, USA), rigid bronchoscope (3.0-4.5) fitting the patient's airway, small caliber grasping forceps (330 mm, R. Wolf 8282.37), suction tip and endoscope charge-coupled device (CCD) camera-monitoring system (Fig. 1).
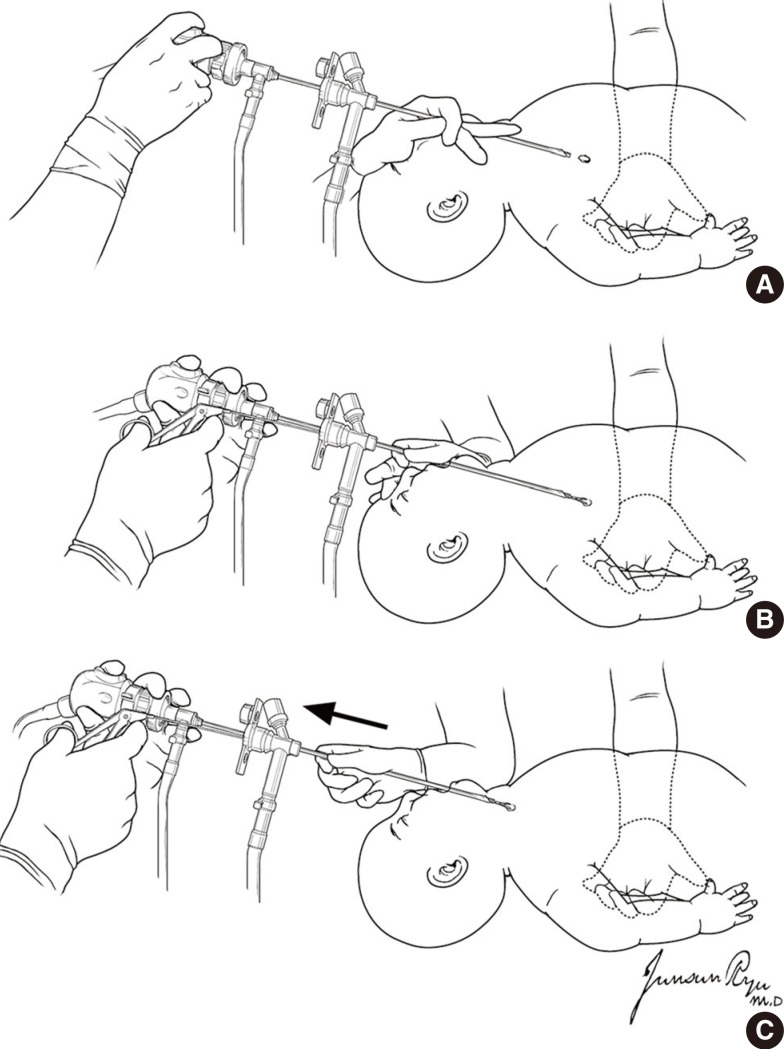
Under general anesthesia, the pediatric patient was positioned supine with the neck extended by an adequate inter-scapular cushion support or the assistant's left hand. Then, the rigid bronchoscope was gently introduced and located at the main trachea followed by a connection of ventilation circuit (Fig. 2). A CCD camera-equipped straight endoscope was introduced through the rigid bronchoscope to visualize the airway. With endoscopic guidance, the operator advanced the rigid bronchoscope along the tracheobronchial tree. At this time, the operator's left hand was holding the rigid bronchoscope and right hand holding the camera-equipped endoscope. Also, the assistant supported the patient's shoulder to make the adequate position and exposure of tracheobronchial tree.
When the bronchoscope approached the site of foreign body impaction, it was positioned in situ by the assistant's right hand. This enabled both of the operator's hands free for manipulation of instruments. Bimanual manipulation involved introducing the grasping forceps through the rigid bronchoscope with one hand while holding the endoscope with the other hand for visualization. To facilitate the dis-impaction of the foreign body while minimizing the damage of mucosa, the foreign body was gently rotated and mobilized by the grasping forceps prior to extraction. All manipulations were done under endoscopic guidance.
After full mobilization of the foreign body, retrieval was accomplished through the retrograde movement of the rigid bronchoscope, endoscope and grasping forceps. The foreign body was carefully and continuously monitored using the endoscope throughout the retrieval process. Special consideration was taken when the foreign body passed through the vocal cord to avoid release from grasping forceps. After the successful retrieval of foreign body, the rigid bronchoscope was re-introduced and the tracheobronchial tree was re-evaluated with endoscopic guidance to confirm the complete removal of the foreign body and airway clearance.
Subjects and retrospective review
From 2003 to 2013, 110 pediatric patients underwent rigid bronchoscopy for suspicious airway lesions. Among them, we selected the pediatric patients <3 years-of-age and diagnosed as foreign body aspiration.
The bimanual endoscope-assisted rigid bronchoscopy (BER) technique, described above, was applied to 29 children and the conventional rigid bronchoscopy (COR) to 33 children. There was no preformed guideline regarding the selection of operative method at the time to perform rigid bronchoscopy. The selection of operative technique had been left upon the operator's preference (comfort and familiarity with using endoscope and equipment) and experience. Meanwhile, the use of each method was equally distributed during the study period. The surgical experience of the operator was less than 2 years (clinical fellows) or 2-5 years (junior faculty) and did not differ between the groups. We retrospectively reviewed the medical records of these patients. The parents submitted a written consent form for use of their medical record, and our Institutional Review Board approved this retrospective review.
The subject characteristics are summarized in Table 1. The outcomes were compared between two groups in terms of operation time and hospital stays (Wilcoxon rank sum test). A two-tailed P-value <0.05 was considered as significant.
RESULTS
The patients were divided into the COR and BER groups in terms of operative techniques. Age distribution was comparable in the two groups (Table 1). A male preponderance was noted in patients with bronchial foreign body in both groups. Cough was a predominant symptom before operation. Other symptoms such as wheezing, dyspnea, fever, and cyanosis were also noted without significant difference between the two groups. Preoperative radiology frequently revealed lung hyperinflation, atelectasis and pneumonic infiltration. Mean duration of the foreign body ingestion was about 9 days in both groups.
Type of foreign body was usually organic materials such as peanuts, or sunflower seeds. Left main bronchus was a more prevalent site of foreign body impaction while appreciable numbers of foreign bodies were located in the right main bronchus. Trachea and segmental bronchus was occasionally noted as a site of foreign body impaction. The surgical experience of the operator did not differ between the groups.
Immediate postoperative chest X-ray showed improved or stationary status compared with preoperative chest X-ray findings while a few patients showed aggravated chest X-ray findings. All foreign bodies but one in the COR group were successfully removed. We performed an in-depth chart review in this case which required multiple procedures. The foreign body was impacted in the left segmental bronchus which complicated the conventional rigid bronchoscopy because of the small sized bronchial lumen, airway edema and mucosal bleeding. Six days after initial failure of retrieval using the conventional technique, the foreign body was successfully removed using the endoscope-assisted approach.
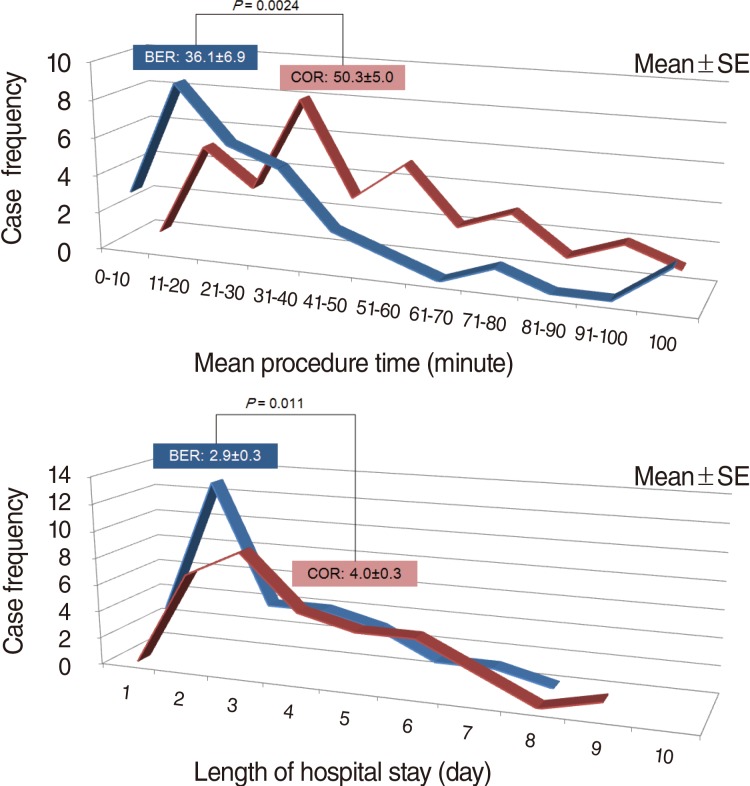
The major differences between the two techniques were the procedure time and length of hospital stay, suggesting easier and more accurate manipulation in the BER procedure (Fig. 3). Patients receiving the BER procedure seemed to recover more rapidly than those treated using the COR procedure.
DISCUSSION
Rigid bronchoscopy is an essential procedure for the diagnosis and treatment for the suspicious airway foreign body [10,11,12]. It provides adequate spaces for manipulation of instruments including grasping forceps and enhances ventilation safety during the procedure [15]. However, the conventional method that relies naked eye may have technical concerns such as blind manipulations of the grasping forceps [13,14]. One can easily imagine that the incorporation of an endoscope system could enhance the visualization and manipulation in the rigid bronchoscopy procedure compared with the use of naked eyes. However, rigid bronchoscopy aided by an endoscope system in very young age has not been well described in the literature. Thus, the purpose of this study is to introduce the detailed step-by-step procedures of an endoscope-guided rigid bronchoscopy and to document its clinical benefits.
The results of our study showed that BER technique is superior to the COR technique in terms of procedure time and hospital stay. Bimanual endoscopic procedure for retrieval of the airway foreign body allowed less traumatic manipulation of instruments during the procedure, which could result in shorter operative time compared with COR. Also, a shortened hospital stay may reflect the earlier recovery in the BER group. Considering that other variables including operator experiences were not different between the two groups, we believe that BER procedure itself has great clinical benefits in very young patients with suspicious airway foreign bodies. In addition, another advantage of an endoscope guided bronchoscopy is a documentation of the procedure, which greatly facilitates education and learning as well as communication.
Optical forceps combining an endoscope with forceps seems to be very useful in managing patients suspected of having airway foreign body [14]. In adult patients, we are currently using the optical forceps (d=3.0-4.5 mm) for the removal of foreign bodies, however in very young age pediatric patients, in which the incidence of the foreign body aspiration is much higher, these optical forceps do not fit into the very small caliber rigid bronchoscope or the manipulation of the optical forceps sometimes can be difficult because of the fixed angle of the endoscope and forceps. Meanwhile, the BER procedure may allow more versatile manipulation of forceps, separately with endoscope movement. However, further studies are needed to compare the clinical efficacy of the BER method with rigid bronchoscopy with 2.9 mm optical forceps.
One curious aspect of this study is higher prevalence of airway foreign bodies in the left main bronchus than in the right side. Airway foreign bodies have been generally known to be aspirated into the right main bronchus due to several reasons including its narrow angle of divergence from the tracheal axis. The reasons are partly because the aspirated foreign bodies can be easily self-expectorated in the right side, or referral to the tertiary center of these patients with foreign bodies in the right side may be less. However, large population-based studies are required for more solid conclusion of this subject.
In conclusion, endoscope-assisted retrieval of airway foreign body and bimanual manipulation of forceps in pediatric patients is superior to the conventional naked-eye method in regard to precise manipulation and safety. In addition, each step we describe here can be applied to the rigid bronchoscopy procedure performed in adult patients.