INTRODUCTION
Currently, smoking is one of the most common addictions among the world's population [1]. Cigarette smoking may affect the smoker in many ways. In particular, it may induce changes in the circulatory and immune systems. Smoking can cause vasomotor dysfunction, induce an inflammatory response in the body, and may modify the lipid profile [2]. The main toxic ingredients of tobacco smoke are various heavy metals [3], notably mercury and arsenic, which can damage hair cells and cause demethylation of nerves in the auditory pathway [4].
In the literature there are many reports of the adverse effects of cigarette smoking on the organ of hearing. In two population-based, cross-sectional studies [56], it was reported that smokers were about 1.5 times more likely to have a hearing loss compared to nonsmokers. Among younger smoking adults there is a higher risk of developing hearing loss later on. Both these studies were adjusted for other risk factors such as noise exposure. Exposure to second-hand smoke may also cause hearing loss in nonsmoking adults [7].
One of the most sensitive tests of hearing is otoacoustic emissions (OAEs), which are low-level sounds originating in the cochlea which can be measured in the ear canal [8]. OAEs require the proper functioning of outer hair cells [9]. Because OAEs are very sensitive to cochlear abnormalities [10], their measurement is an excellent tool for monitoring cochlear status, such as after application of ototoxic drugs [11] or exposure to noise [12].
There are a number of studies of OAEs in relation to smoking. In the study of Paschoal and Azevedo [13], it was shown by measuring transiently evoked OAEs (TEOAEs) that a group of smokers had a lower response at 1 kHz in both ears. Among smokers there were more cases of tinnitus. Also in the studies of Vinay [14] and Mustafa [15], overall TEOAE amplitude was significantly reduced in smokers compared to nonsmokers.
When studying distortion product OAEs (DPOAEs) a small, but significant, decline in DPOAE levels in smokers compared to nonsmokers has been shown [16]. Input/output detection thresholds are also significantly elevated at high frequencies in smokers as compared to nonsmokers.
In the research of Durante et al. [17] children exposed to tobacco smoke were examined. Their TEOAEs showed lower response levels, mainly at frequencies of 2-2.8 kHz, and lower signal to noise ratios (SNRs), mainly at 1-1.4 kHz, when compared to controls that were not exposed to tobacco smoke. The average reduction in TEOAEs of children exposed to tobacco smoke was 2.1 dB. Also in neonates whose mothers had smoked during pregnancy the average response levels were lower compared to neonates whose mothers had not smoked [1819]. Interestingly, changes in OAEs may be apparent even before there is an evident decline in audiometric thresholds up to 20 kHz [16]. These studies confirm a relationship between cigarette smoking and hearing loss.
In some ears spontaneous OAEs (SOAEs) can be observed [20]. SOAEs are usually an indicator of very good hearing [21]. Ears with SOAEs also have higher levels of evoked OAEs [2223], regardless of audiometry [24].
This study aimed to determine whether and how cigarette smoking affects OAEs in a population of young smokers with normal hearing. TEOAEs, DPOAEs, and SOAEs were analyzed in search of some preclinical changes.
MATERIALS AND METHODS
OAEs were recorded from the ears of 48 young adults (age, 20 to 27 years). The dataset was divided into two groups: smoking (12 women and 12 men) and nonsmoking (12 women and 12 men).
This study was performed according to the Declaration of Helsinki. The research procedures were approved by the Ethics Committee of the Institute of Physiology and Pathology of Hearing, Poland. The subjects gave written informed consent prior to participation. An interview excluded those with hearing disorders that could affect the results. Questions involved a self-evaluation of their hearing status, present and past hearing problems, ear, nose, and throat (ENT) diseases, ear surgery, chronic diseases, ototoxic medication now and in the past, hormonal medication by women, and exposure to noise. They were also asked whether they smoked or not, and each smoker was asked about the number of cigarettes smoked and how long they had smoked. In this way we determined the average number of cigarettes smoked per day (8.7 cigarettes; range, 1 to 20 cigarettes) and the average time they had smoked (3.8 years; range, 1 to 8 years). In further analyses the amount of smoking is described by pack-years. This measure was introduced in earlier studies [25] and is defined as the number of packs of 20 cigarettes smoked per day, multiplied by the duration of smoking in years. The average pack-year in the smoking group was 1.8±1.5.
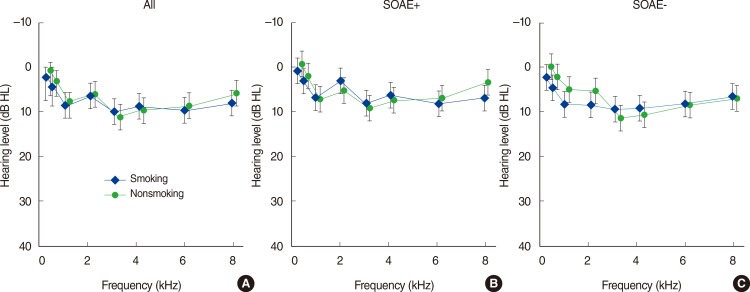
All subjects were laryngologically healthy and had no otoscopic ear abnormalities. Impedance audiometry gave normal type-A tympanograms and normal acoustic reflexes. Average hearing thresholds (Fig. 1A) were better than 20-dB hearing level for all test frequencies (0.25, 0.5, 1, 2, 3, 4, 6, and 8 kHz). The two groups did not differ significantly in terms of audiometric thresholds.
OAE measurements were made using the ILO 292 device (Otodynamics Ltd., Hatfield, UK). In each ear three OAE measurements were made: TEOAEs, DPOAEs, and SOAEs. TEOAEs were recorded using the nonlinear protocol, stimulus levels were kept at the standard default settings of 78- to 82-dB peak sound pressure level (SPL), the recording window was 20 ms, and there were 260 subaverages. Half-octave-band values of OAE SNRs and response levels were used for analyses. DPOAEs were measured with stimulus levels of 65 and 55 dB using an f2/f1 ratio of 1.22, and at frequencies of 1, 1.4, 2, 2.8, 4, and 6 kHz.
SOAEs were acquired using the inbuilt technique provided by the ILO 292 equipment, resulting in measurement of so-called synchronized SOAEs (SSOAEs). An ear was classified as "with SOAEs" when at least one long-lasting peak was found in the SSOAE spectrum that exceeded the noise floor by 5-dB SPL.
For all parameters the statistical significance of the mean difference between groups was evaluated using the Wilcoxon rank sum test. This is equivalent to Student t-test when the analyzed populations do not have normal distributions. Pearson correlations were used to evaluate some relationships. In all analyses, as a criterion of significance, a 95% confidence level (P<0.05) was chosen.
RESULTS
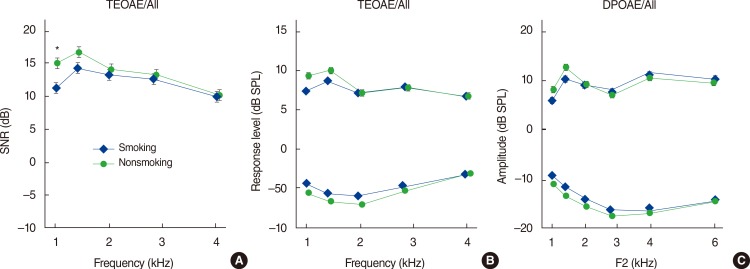
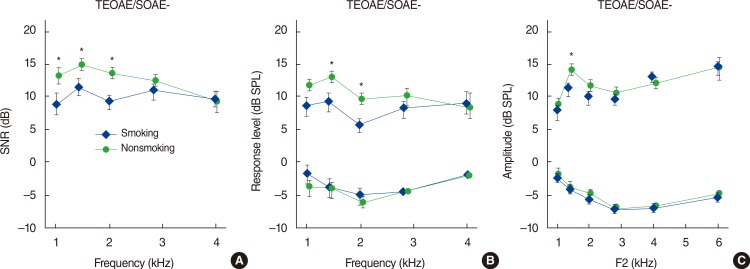
As mentioned, the average pack-years in the smoking group was 1.8±1.5. In Fig. 2, response levels and SNRs for TEOAEs and DPOAE levels are shown for the ears of smokers and nonsmokers. Average evoked OAE data initially did not reveal appreciable differences between the groups. The only significant difference was for TEOAE SNRs in the 1-kHz band. There was no significant difference for DPOAEs in any band. To look for more subtle effects we focused on SOAEs. Ears were divided into two groups according to whether or not they had SOAEs. The numbers of ears with and without SOAEs are given in Table 1, while pure tone audiometry results are shown in Fig. 1B, C, respectively. The average pack-years of the subgroup with SOAEs was slightly lower (1.7±1.3) than that of the subgroup without SOAEs (2.0±1.9), but there was no statistically significant difference between them. In Figs. 3, 4, the data are presented in a similar manner to Fig. 2, but for ears with (Fig. 3) and without SOAEs (Fig. 4). Of the ears that exhibited SOAEs, both smokers and nonsmokers, there were no statistically significant differences in terms of TEOAEs and DPOAEs (Fig. 3). There was also no significant difference in audiometric results. However, Fig. 4 shows that, in all ears without SOAEs, evoked OAEs were higher by as much as 5 dB at certain frequencies in the ears of nonsmokers compared to smokers. These differences were most prominent in the 1- to 2-kHz range. However, there was still no significant difference in audiometric results. In the case of TEOAEs, statistically significant differences in response levels were found in the 1.4- to 2-kHz range (P<0.05). TEOAE SNRs were lower for smokers in the 1- to 2-kHz range (P<0.05). For DPOAEs, a significant difference occurred only at 1.4 kHz (P<0.05), while there was no statistically significant difference in the noise floors.
Additionally it can be observed that, within both smokers and nonsmokers, evoked OAE parameters of ears without SOAEs were also lower in comparison with ears with SOAEs. These differences were more prominent for smokers: significant differences in TEOAE response levels were seen at 1-2.8 kHz and for SNRs at 1-2 kHz (P<0.05). In the case of DPOAEs in smokers, a significant decrease in levels in ears without SOAEs was evident at 1.4-2 kHz (P<0.05). At 2 kHz this decrease coincided with an audiometry decrease (P<0.05). For nonsmokers, there was generally no statistically significant difference in TEOAE response levels, SNRs (except at 1.4 kHz, P<0.05), or DPOAEs (except at 1 kHz, P<0.05). For nonsmokers there were also no significant differences in pure tone audiometry between ears with and without SOAEs.
The incidence of SOAEs is summarized in Table 1. Of all the ears of smoking subjects there were 29 that had SOAEs, similar to nonsmokers where there were 32. Their evoked OAEs (as seen in Fig. 3) were also comparable to those of nonsmokers. Of course, there were cases where a smoking person had very good hearing, high levels of evoked OAEs, and many SOAEs. However, in general the number of SOAEs decreased with number of pack-years (r=-0.2, P<0.05). For example, there was one person who had 10 SOAEs in her left ear and 5 in her right, but she smoked only 1.05 pack-years. Another person smoked 3.75 pack-years and had 1 SOAE in the left ear and 3 SOAEs in the right. The person who smoked the highest number of pack-years (6) in this study did not have any SOAEs.
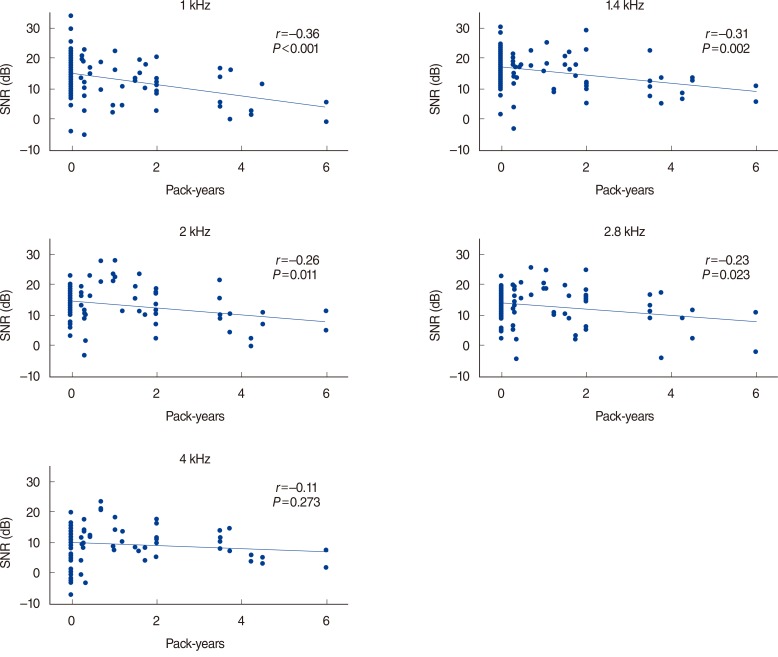
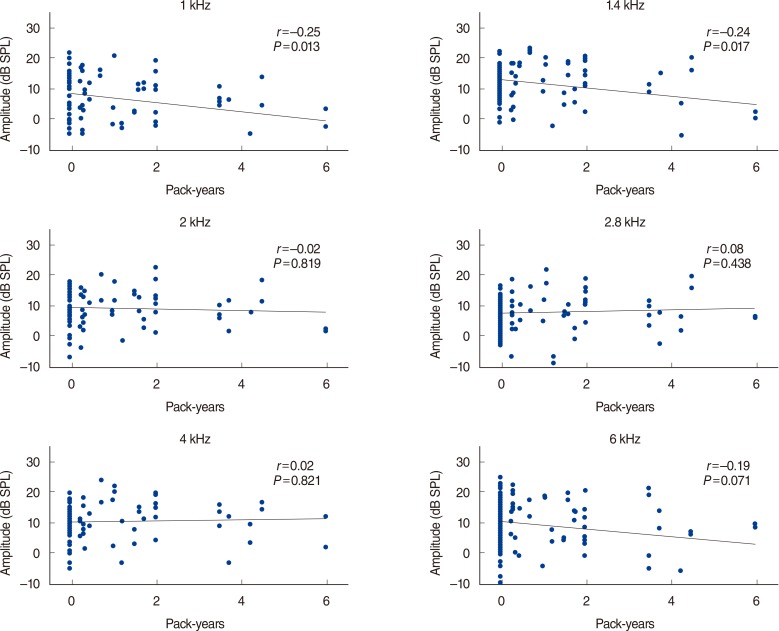
Finally we tried to assess if the amount of smoking had any significant effect. As mentioned in the "MATERIALS AND METHODS" section, there were no significant differences between groups in terms of pure tone audiometry at any frequency. Also audiometric results did not correlate with amount of smoking. On the other hand, both TEOAE response levels and SNRs were negatively correlated to pack-years (Figs. 5, 6). The correlations were significant but weak in the 1- to 2.8-kHz range (rε[-0.36 -0.20], P<0.05). Also DPOAEs (Fig. 7) weakly correlated with pack-years at 1 and 1.4 kHz (r=-0.25 and r=-0.24, P<0.05). As the smoker group was relatively small we divided it into two subgroups according to the median number of pack-years (1.55). The first group smoked less than or equal to 1.55 (24 ears), and the second more than 1.55 pack-years (24 ears). It was found that the evoked OAE parameters, and average number of SOAEs per person, were smaller in the second group. Fig. 8 shows TEOAE response levels, SNRs, and DPOAE levels. SNRs were significantly smaller by as much as 4 dB in the frequency bands 1.4-2.8 kHz (P<0.05). A significant difference in response levels occurred only at 2.8 kHz. There were no significant differences in DPOAEs. The average number of SOAEs per person decreased from 3.1±3.2 to 1.0±1.2 (P<0.05).
DISCUSSION
The motive for this study was to search among young adults for minor, preclinical effects of smoking on OAEs. All subjects in the studied group had normal hearing thresholds. The longest reported amount of smoking was 6 pack-years, but many subjects smoked less than 1 pack-year.
When comparing the group of smokers with the control group, differences in OAE parameters were initially found only for 1 kHz. However, more changes came to light when the presence of SOAEs was taken into account. When TEOAEs from the ears of smokers without SOAEs were compared with those of the control group, significant decreases were found at 1-2 kHz. In general, levels and SNR of evoked OAEs and number of SOAEs were negatively correlated with pack-years. In the study of Paschoal and Azevedo [13], a decrease in TEOAEs was found at 1 kHz, similar to the present study. Decreases in TEOAE amplitudes have been found in smokers compared with nonsmokers in some other studies [1415]; however, in these cases only the overall response was taken into account, without analysis of frequency bands.
Turning to DPOAEs, in the present study a general decrease was detected in ears without SOAEs of smokers, but the only significant difference was at 1.4 kHz. This differs from previous studies that found changes at higher frequencies. In the study of Negley et al. [16], a reduction in DPOAEs was found in the 2- to 8-kHz range. In the study of Torre et al. [26], a similar frequency range was studied for a group that had slightly less cigarette use; a reduction in levels was observed but it was not statistically significant. In both these studies, frequencies below 2 kHz were not studied. The discrepancies between the present work and previous results might be due to the longer smoking periods in the two previous studies: in the study of Negley et al. [16] subjects had smoked for 5-8 years, and in the study of Paschoal and Aze-vedo [13] for more than 1 year (although the authors do not provide exact figures for the amount of exposure [1316]). In the present study the length of smoking and number of pack-years (0.25-6) was relatively small. In studies that have demonstrated changes in pure tone audiometry the number of pack-years was usually more than 10 [5]. The effect of smoking is especially clear for people that smoked 30-40 pack-years [527].
The origins of SOAEs are still unclear. We do not know why some people with good hearing have them and some do not. Nevertheless it is now generally accepted that SOAEs correlate with good hearing [21]. In this study there were some smokers who had SOAEs and high levels of TEOAEs and DPOAEs. So it seems there is no immediate damage to the inner ear caused by nicotine. The explanation may be that these people generally had very good hearing and, given their relatively young age and short smoking time, no pathological changes had yet developed.
We interpret our results as follows. SOAEs are usually present in ears with acute hearing [21]. Even if a person is a smoker, if his or her ears exhibit SOAEs there will be no signs of deterioration. Possibly it is too early for the effects of nicotine toxicity to show up. In comparison, ears without SOAEs have begun to show a significant decrease in evoked OAEs, even for comparable amount of smoking. It would be very interesting to study smokers with SOAEs after some time, to check if these ears finally show signs of deterioration and particularly if there are any changes in SOAEs. In fact, some studies have already shown that there is a relationship between the presence or absence of SOAEs and negative effects on hearing, even when there are no measurable differences in audiometry (e.g., for tinnitus patients [28]).
To conclude, even relatively short periods of smoking can have negative effects on hearing, i.e., cause measurable decreases in OAE levels. Ears that do not exhibit SOAEs seem to have sustained some damage, while ears with SOAEs seem to be intact, at least initially. TEOAEs seem to be more affected by smoking than DPOAEs. Longitudinal studies are needed to confirm these ideas.