INTRODUCTION
Radical treatments are part of the management of refractory, disabling vestibular disorders, such as MeniereŌĆÖs disease that are resistant to more conservative measures [1-4]. Intratympanic (IT) gentamicin injections is a well-recognized method for managing patients with unilateral MeniereŌĆÖs disease [1-3], while labyrinthectomy, although more invasive, has also been used as definite treatment [3,4]. Both treatment options can ablate the vestibular function; however, the IT gentamicin injections have the significant advantage of expected hearing preservation, particularly in patients with serviceable hearing [1-4].
Lately, a very few studies have looked into the precise impact of gentamicin on the injected ear using vestibular tests, including the relatively newly introduced six-canal video-head-impulse test (vHIT) [5-10]. The six-canal vHIT offers a fast, noninvasive measurement of the function of each individual semicircular canal [9,10]. Using vHIT, previous studies managed to show the impact of IT gentamicin injections on the semicircular canals, confirming its vestibulotoxicity, highlighting that one IT injection might not be enough to ablate the ipsilateral vestibular function [5,7-9]. When it comes to labyrinthectomy, studies assessing the vestibular function are missing, mostly because it is assumed that following the surgical intervention no function is preserved. Additionally, the impact of either chemical or surgical ablation on the vestibular response of the contralateral ear has barely been investigated [11,12]. As such interventions ablate function completely on the applied side, any impact on the only remaining functional ear can be detrimental.
There is a lack of studies assessing the result of IT gentamicin injections and/or labyrinthectomy to the contralateral, ŌĆ£healthyŌĆØ ear. Given the potential clinical significance of any abnormalities caused in the remaining functional ear, we aimed at investigating the impact of both IT gentamicin injections and labyrinthectomy on the contralateral ear using six-canal vHIT; we also examined the order that gentamicin ablates the semicircular canals.
MATERIALS AND METHODS
Basic settings
A pilot, qualitative, observational study was carried out in a tertiary, referral, university center. Ethical approval was granted by the Institution Audit Board. Informed consent was obtained by all enrolled patients.
Patient selection
We enrolled patients with unilateral vestibular pathology without any response to conservative, nonablating methods and/or with a medical indication for radical treatment. Following detailed consultation and meticulous individual assessment we organized the patients into two groups; group I consisted of patients undergoing IT gentamicin injection and group II patients undergoing labyrinthectomy, without any preoperative IT gentamicin application. None of the patients had known contralateral ear disease. Patients who would potentially benefit from either intervention were offered both options and were treated with the method of their choice.
Group I included seven patients treated with IT gentamicin application; three patients with unilateral MeniereŌĆÖs disease and four patients with vestibular schwannoma, planned for translabyrinthine resection, as part of the prerehabilitation management scheme utilized in our department. Group II consisted of six patients; three patients undergoing a translabyrinthine resection of a vestibular schwannoma, one to obtain clear margins in temporal bone malignancy, one to remove petrous apex cholesteatoma and one for MeniereŌĆÖs disease following failure of IT steroid injections (patient declined any further IT treatment). All patients from both groups underwent six-canal vHIT in predetermined time intervals.
IT gentamicin injections and labyrinthectomy
All IT injections were performed in the same standardized way by the same surgeon; the number of injections required ranged from two to three with 1-week interval between the injections; enough time to assess the patient clinically, perform vHIT and decide if additional injections were required.
A 40 mg/mL solution of Gentamicin was utilized with approximately 0.6ŌĆō0.8 mL of solution instilled into the middle ear via a 22-G spinal needle under topical anaesthesia using the surgical microscope. The patients were asked to keep their head turned towards the contralateral side for 30 minutes after the injection. The labyrinthectomy took place in the same tertiary center, performed in also a well-described standardized way until the complete labyrinth including the three semicircular canals, the vestibule and the ŌĆ£bony islandŌĆØ had been drilled away.
Six-canal vHIT
Six-canal vHIT were performed by experienced, subspecialized audiologists using the Otometrics six-canal vHIT device and software (Otometrics, Taastrup, Denmark) in a targeted velocity of >200┬░/sec to ensure accurate, reproducible results. A vestibular-ocular reflex gain between 0.8 and 1.2 was considered normal [9]; we additionally analyzed the raw data, including covert and overt saccades for each semicircular canal to identify abnormal responses.
The patients in group I underwent preoperative vHITs as well as 3 to 5 days following each injection to monitor their response to gentamicin and ensure that pharmacological ablation of the labyrinth had been achieved. We documented the order that each canal responded to gentamicin for every case until all canals had been ablated.
The labyrinthectomy group also had baseline vHIT conforming preoperative normal contralateral responses. Following surgery all patients underwent postoperative six-canal vHIT, 12 to 42 weeks postoperatively at the stage when the patients had no imbalance symptoms and were fit for such testing. All patients from group II were clinically assessed 6 weeks, 12 weeks, 6 months and 12 months following the treatment but vHIT was performed when they were clinically fit and asymptomatic.
Outcome measures
Our main outcome measures were the contralateral semicircular canal responses on vHIT. We documented the vHIT gain for each individual canal, on both the ipsilateral and contralateral side in cases of IT gentamicin injection and on the contralateral side in cases of labyrinthectomy; we also analyzed the raw data looking for covert and/or overt saccades. Additionally we documented demographic factors. We did not include hearing data, mainly because this was not the aim of our study but also because many of the patients were already suffering from severe to profound hearing loss prior to intervention; thus hearing was not tested following IT gentamicin injections. As expected, no measureable hearing was detected ipsilaterally following the labyrinthectomy.
For the patients in group I, we also documented the gain/abnormal response for each canal following every injection in order to determine the precise order that the canals respond to IT gentamicin application. We did not randomize our patients because of the heterogeneity of the groups and because we felt it was not ethical to do so.
RESULTS
Demographics
A total of 13 patients, four males and nine females, were enrolled in this study; seven patients underwent IT gentamicin injection and six labyrinthectomy (Table 1). The average age for the patients in group I was 45.9 years (range, 27 to 66 years) while for group II 47 years (range, 25 to 70 years).
Responses from the ipsilateral side
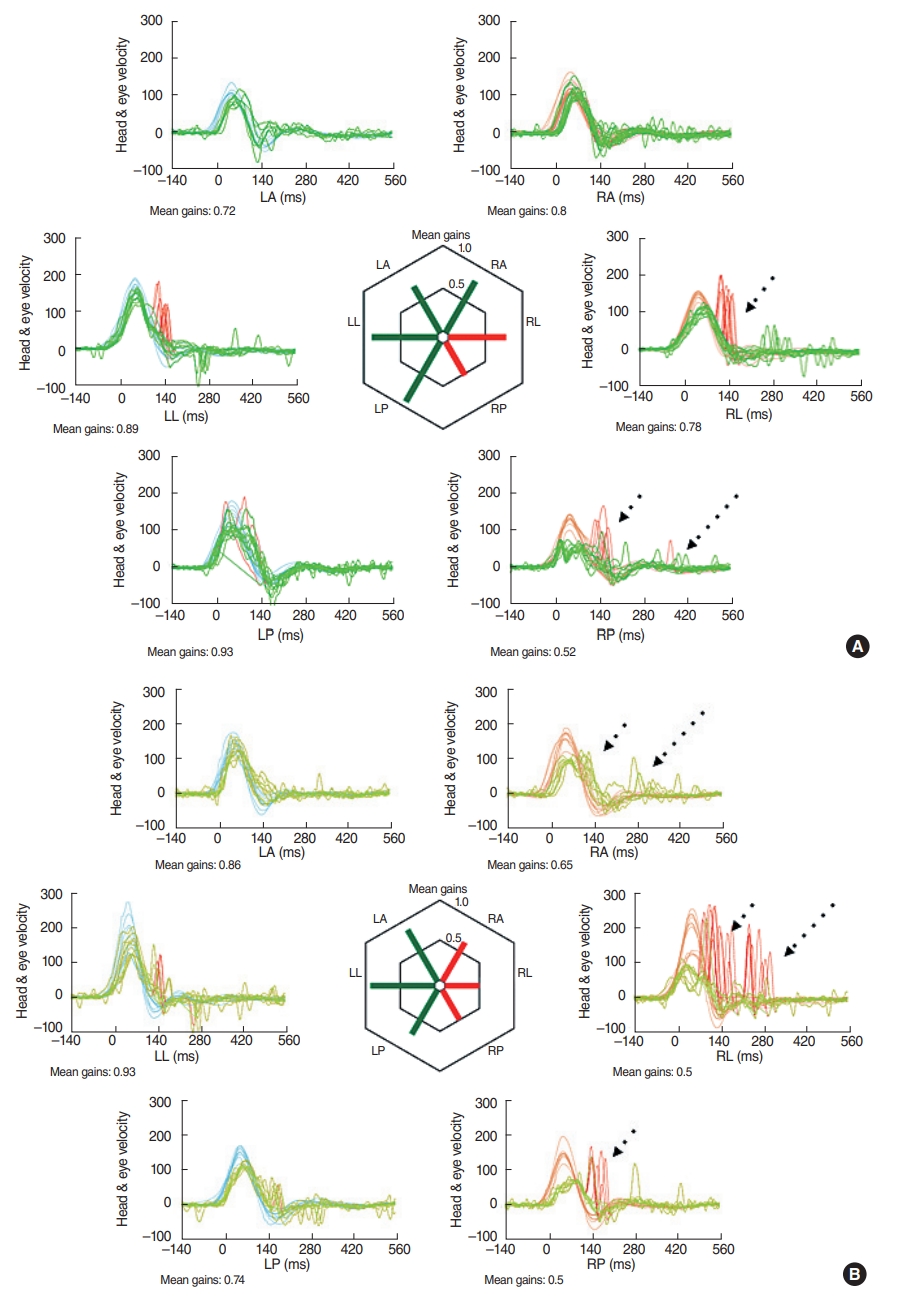
From group I, as expected, all patients had abnormal gain and responses in the raw data from the ipsilateral ear, following labyrinthectomy. From group II, in all patients ablation of all three ipsilateral canals was achieved following two to three injections (average 2.4 injections). Following the first IT injection, the lateral semicircular showed abnormal gain in six out of seven ears (85.7%), while the posterior semicircular canal in four out of seven (57%) and the superior in one out of seven (14.3%). Following the second injection, the lateral and the posterior canals were ablated in all cases (100%), while the superior in five out of seven (71.4%). A third injection was required in two patients to ablate the superior semicircular canal. We had no patients with three-canal response to just one injection. Only in one patient the superior canal responded before the posterior; in all cases the lateral canal responded first to gentamicin. In summary, the lateral semicircular canal was the most sensitive to IT gentamicin injections followed by the posterior canal. The superior is usually ablated last (Fig. 1).
Responses from the contralateral ear
None from the patients from group II had abnormal responses from the contralateral ear, either following each injection or after the complete ablation. In particular, the raw data from the contralateral ears were normal for the patients treated with IT gentamicin injection without any convert or overt saccades (Table 2).
On the other hand, patients in group I undergoing labyrinthectomy had abnormal responses from at least one contralateral semicircular canal, with abnormal gains and coverts/overt saccades (Table 2). Only in one patient, the vHIT gains from the contralateral ear were within normal range; however, analysis of the raw data, showed abnormal responses (covert saccades) from the contralateral lateral semicircular canal.
DISCUSSION
IT gentamicin injections and labyrinthectomy have both been used over the years to treat disabling, unilateral vestibular disease, while the labyrinthectomy has also been used to access and remove temporal bone/skull base pathology. The impact of such interventions on the affected ear is definite and irreversible [1-4]. However, their effect on the contralateral, healthy ear has not been investigated, until now. We present, to our knowledge for the first time, abnormal, repeatable responses recorded from the contralateral ear in all enrolled individuals undergoing labyrinthectomy; on the other hand, none of the patients treated with IT gentamicin application had any contralateral abnormal responses. We additionally, demonstrated in vivo, the order that the semicircular canals respond to IT gentamicin injections, with the lateral one being the most sensitive and the superior one the most resistant.
The significance of contralateral responses
To date, the impact of unilateral vestibular deafferentation on the contralateral labyrinth and the central system has been poorly examined and understood. An older study showed reduced vestibular-ocular reflex gain in the contralateral ear immediately after labyrinthectomy in monkeys, with later recovery [11]. Additionally, recent work investigating contralateral vHIT responses following retrosigmoidal vestibular schwannoma resection showed the same short-term reduction in gains followed by gradual stabilization [12], while previous work reported no long-term recovery at all, in certain patients [13]. Our study shows similar results following surgical labyrinthectomy with abnormal contralateral responses several months following the initial intervention. We did not perform any immediate measurements like Mantokoudis et al. [12] because of the practical challenge of performing six-canal vHIT following major surgery; therefore we were unable to assess the immediate postoperative function; however, the abnormal gain was evident in all patients following labyrinthectomy in at least one canal many months down the line. Of note that in our study we tested all six canals and not only the lateral one.
One could assume that in the three patients who underwent labyrinthectomy for a vestibular schwannoma resection, additional vestibular nerve sacrifice was performed to remove the tumor with such procedure adding to the vestibular trauma. However, the same results were recorded in the other three patients who did not have any intervention on the vestibular nerve. Thus, the responses generated by the contralateral ear are more likely the result of the labyrinthectomy rather than any additional manipulations.
The reason behind such abnormal responses is difficult to prove. However, a process of on going central compensation is a likely plausible explanation. Indeed, the previously reported hypothesis of inhibited contralateral vestibular pathway by the central nervous system as part of central compensation following acute vestibular damage is a possible explanation [12,14].
On the other hand, we did not identify any contralateral gain changes following IT gentamicin injections, despite the ipsilateral reduced gains documented in all three canals. Although the precise, underlying mechanism of such finding is not entirely clear, we hypothesize that it might reflect the gradual impact of gentamicin on the labyrinth and the central compensation mechanisms, in contrast to the sudden and rapid damage achieved through surgery. Interestingly, the vHITs were performed much later in the labyrinthectomy group, which gave the patient more time to compensate. Still, though, these patients demonstrated abnormal contralateral responses, while the patients from the gentamicin group, tested only five days post-injection (in theory less time to compensate), did not produce any contralateral abnormal responses.
Another possible explanation could be that the reduced ipsilateral gains following IT gentamicin application do not necessarily mean that there is no remaining ipsilateral vestibular function, while in case of labyrinthectomy there is no remaining function at all. Such ŌĆ£less traumaticŌĆØ impact of IT gentamicin is still able to improve the patientsŌĆÖ symptoms by reducing the ipsilateral vestibular function rather than completely ablating it; consequently it generates milder contralateral responses. Indeed, the presence of covert and/or overt saccades is part of the compensation mechanism as a response to unilateral vestibular deafferentation [12,15]. The lack of such contralateral saccades following IT injections but their presence after labyrinthectomy indicate a milder and possibly more gradual impact of gentamicin compared to the rapid and sudden damage caused surgically.
Interestingly, Roehm et al. [16] reported traces of gentamicin in the contralateral ear in chinchillas following IT gentamicin injections. The authors attributed this transfer of gentamicin from one side to the other to the cochlear aqueduct [16]. Our study did not examine traces of gentamicin on micro-level; only vHIT responses from the contralateral ear, which in the gentamicin group were all normal. Whether there is transfer of gentamicin to the contralateral ear via the cochlear aqueduct in the human ear, it is unknown. The normal contralateral responses shown in our study suggest that even if such transfer occurs in human, it is probably not sufficient enough to cause abnormal vHIT results.
To our knowledge, there is a lack of similar studies in the literature; our work offers the first direct comparison of labyrinthectomy and IT gentamicin injections. Additional studies will be of benefit for shedding more light on the indirect impact of radical interventions on the contralesional side and the central compensation mechanisms.
Semicircular canal responses to IT gentamicin
We have shown a relative resistance of the superior canal to IT gentamicin injection, while the lateral canal was the first one to show abnormal gain, followed by the posterior. Such finding is probably related to the anatomy. Indeed, following IT injection, the gentamicin enters the inner ear through the round and oval windows. Given the horizontal, slightly elevated position of the patientŌĆÖs head, the lateral semicircular canal is the first one to be affected. On the other hand, because of gravity the superior canal can be expected to respond last.
Marques et al. [17] found reduced ipsilateral gain in all canals following one IT gentamicin injection in some patients. As shown by previous study looking into the ototoxicity of systemic gentamicin, such agent can be vestibulotoxic in any dose and in any regime [8]. Thus, there should be patients who will respond to even one IT gentamicin injection without the need for a repeat application. We did not record similar responses, as we had no case with abnormal responses in all three ipsilateral canals following just one injection. This might be either because of the enrolled numbers or even related to the method of IT application and the presence of middle ear related factors such as adhesions. However, the ipsilateral vestibular-ocular gains finally reduced in all canals following a maximum of three injections.
Strengths and limitations
The novelty and the prospective structure of our work are its main strengths. This is the first study directly comparing the impact of IT gentamicin application with the impact of labyrinthectomy on the contralateral side. At the same time, using six-canal vHIT we showed the order that the canals respond to IT gentamicin injections. Utilizing the six-canal vHIT technique allowed us to assess all canals in an accurate way, as it has been proven as a quick and repeatable way of assessing all six semicircular canals [8,12,18,19].
The main limitation of the study is the relatively small number of the enrolled patients. Additionally, we did not randomize our patients because of the heterogeneity of the groups and ethical considerations when offering radical interventions. However, this is a pilot study involving radical unilateral vestibular ablation as part of an on going time-demanding project on vestibular assessment; thus we did not include audiological outcomes (radical treatments, profound/complete hearing loss). The tertiary settings that allowed us to recruit individuals and also to perform the interventions and the repeated six-canal vHITs in a controlled environment ensure accurate results and careful data interpretation, helping us to overcome the limitation of small numbers.
Our study shows abnormal responses from the contralateral ear following labyrinthectomy even many months following the treatment. On the other hand, IT gentamicin does not generate such responses while at the same time it achieves the desired ipsilateral reduced vestibular response, making it a radical treatment of choice compared to labyrinthectomy for unilateral vestibular dysfunction. Finally, IT gentamicin seems to affect the ipsilateral canals in a certain order with the lateral semicircular canal being the first one to be ablated.
HIGHLIGHTS
Ō¢¬ Six-canal video-head-impulse test shows that osseous labyrinthectomy causes abnormal contralateral vestibular responses, while chemical ablation of the labyrinthine function with intratympanic gentamicin injections does not.
Ō¢¬ Both, surgical labyrinthectomy and chemical ablation with gentamicin result in ipsilateral abnormal or non-recorded vestibular function, as expected.
Ō¢¬ Intratympanic gentamicin ablates first the lateral semicircular canal; the superior semicircular canal, possibly because of gravity, is the last one to be affected.