INTRODUCTION
Olfaction is one of the most primitive senses when considered in the context of evolution. Approximately 400 genes code for olfactory receptors in the human genome, accounting for 2.4% of the entire genome and constituting the largest gene family [1]. Until recently, it was a common belief that the human ability to smell is inferior to that of other mammals, primarily due to the small size of the olfactory bulbs compared to the entire brain. However, studies have suggested that although the relative olfactory bulb size and the number of olfactory receptor coding genes fall behind those of rodents, humans have an olfactory system with complex networks and pathways that allow us to perform as well as or even better than some other mammals [2]. A study that examined the resolution of human olfaction calculated that humans can discriminate at least 1 trillion olfactory stimuli [3]. Although we may not realize it, our behavior is strongly influenced by the sense of smell, and the decisions we make may often be driven by the nose telling us what to do [4]. Olfaction starts in the womb, as the developing fetus reacts to olfactory stimuli at around 30 weeks. The fetus becomes familiar with the components of the maternal diet, which are transferred via the amniotic fluid [5]. The development of olfaction is vital in bonding between infants and mothers [6]. Olfactory dysfunction can also lead to malnutrition, from a distorted sense of smell and taste resulting in diminished enjoyment of food [7]. The sense of smell can impact one’s survival, as some odors, such as gas leaks, spoiled food, or smoke, can provide warning signs. A study showed that olfactory dysfunction in the elderly is one of the strongest predictors of 5-year mortality, although this certainly reflects correlation and not causation [8]. Olfactory neurons have the ability to regenerate, and recent studies on olfactory training have shown that olfactory function can be improved through practice [9]. After Buck and Axel were awarded the Nobel Prize in Physiology or Medicine in 2004 for their work on odorant receptors and the olfactory system [10], olfaction has attracted considerable interest from researchers in various fields. Olfactory dysfunction in neurodegenerative diseases, including Parkinson disease (PD) and Alzheimer disease (AD) is one of the earliest signs of the impending cognitive impairment. Recently, during the coronavirus disease 2019 (COVID-19) pandemic, smell and taste loss have been well recognized as one of the key symptoms of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection [11,12]. This has raised interest in olfaction and taste among both physicians and the general public. In this review, we outline the essentials that otorhinolaryngologists should know when they manage patients with olfactory dysfunction and help patients, including the basic anatomy and physiology of the olfactory system and related diseases.
EPIDEMIOLOGY OF OLFACTORY DYSFUNCTION
Depending on the method of evaluation, studies report varying prevalence of olfactory dysfunction, from as low as 1.4% to as high as 62.4% [13]. In the US and Korean Health and Nutrition Examination Surveys, the prevalence of olfactory dysfunction has been estimated to be about 10% to 14% and 4.5%, respectively [14-16]. A systematic review and meta-analysis investigating the prevalence of olfactory dysfunction in the general population reported the overall prevalence to be about 22.2% [13]. While olfactory function can change suddenly from some etiologies, other etiologies can cause it to decline slowly over time. In these cases, one may not perceive the severity until there is no function (anosmia). Thus, the actual prevalence of olfactory dysfunction is expected to be higher than those estimated by self-reports in surveys. In the analysis by Desiato et al. [13], the prevalence was 28.8% when determined by objective testing, which was significantly higher than the rate of 9.5% determined by subjective means.
TYPES AND CAUSES OF OLFACTORY DYSFUNCTION
Olfactory dysfunction can be described as qualitative or quantitative in nature. Hyposmia (a diminished sense of smell) and anosmia (the complete inability to sense odors) belong to the quantitative category. Qualitative dysfunction, which is usually accompanied by quantitative dysfunction, consists of parosmia (a distorted sense of smell) and phantosmia (sensing an odor that is not present). Infectious diseases, such as upper respiratory viral infections, and inflammatory diseases such as chronic rhinosinusitis, especially with polyposis, can cause olfactory dysfunction [17]. In these cases, olfactory dysfunction can be both conductive and sensorineural [18]. Conductive-type olfactory dysfunction results from airflow blockage that prevents odorants from binding with the olfactory sensory neurons while damage or disorder of the olfactory sensory neurons or the olfactory pathways results in sensorineural-type olfactory loss. Rhinologic diseases, such as chronic rhinosinusitis with nasal polyps, can cause both conductive and sensorineural-type olfactory dysfunction. Patients with neurodegenerative diseases such as AD or PD can also present with gradual-onset olfactory loss [19]. Trauma, neoplasms, congenital anosmia, medications and toxins, metabolic and endocrine disorders, normal aging, and many other factors can also be etiologies of olfactory dysfunction. According to previous studies, post-infectious olfactory dysfunction (PIOD) is one of the most common causes of olfactory dysfunction [20]. As smell and taste loss have been identified as symptoms of SARS-CoV-2 infection, many are now realizing the importance of olfaction in health and quality of life [11].
ANATOMY AND PHYSIOLOGY OF OLFACTION
The sense of smell
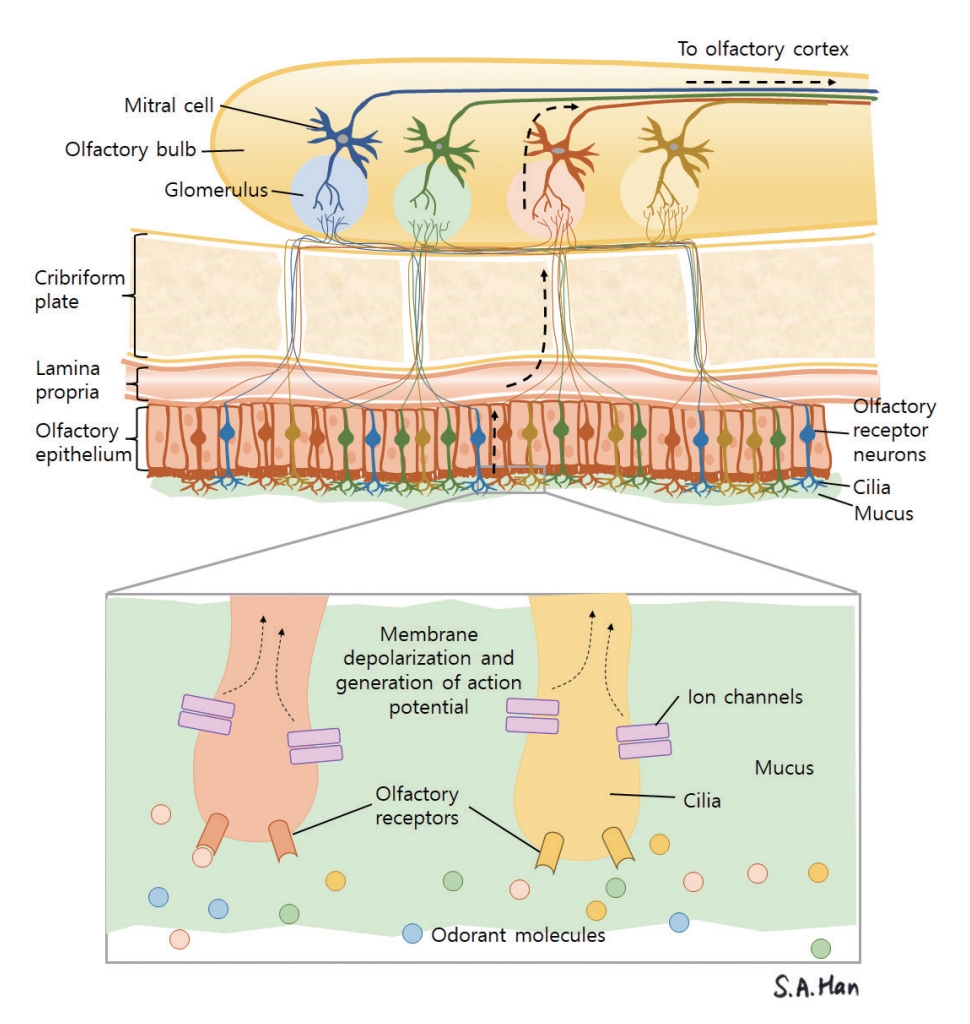
Of the five basic human senses, smell and taste are chemical senses. Olfactory receptor neurons act as distant chemoreceptors that sense odorant molecules. Odorant molecules in the air come in contact with the olfactory mucosa in two ways. The first is through the orthonasal pathway, in which odorant molecules pass through the nasal vestibule into the nasal cavity via airflow. The second pathway involves odorant molecules being transported to the nasal cavity in a retrograde fashion through the nasopharynx from the oral cavity and oropharynx [21]. After the odorant molecules dissolve into the mucus lining the olfactory mucosa, the molecules bind to olfactory receptor neurons, resulting in depolarization and the relay of action potentials [22]. These action potentials are delivered to the olfactory bulb and are relayed to the olfactory cortex through the olfactory tract (Fig. 1) [23].
Structure of the olfactory mucosa
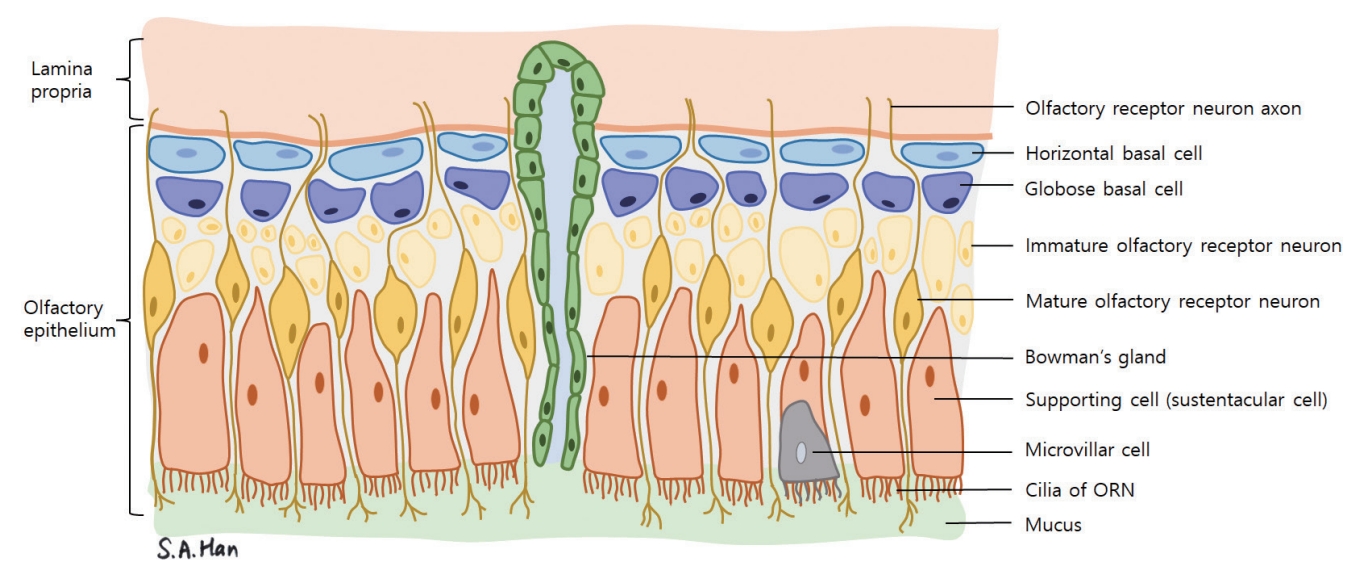
The structure of the olfactory mucosa can be differentiated from the respiratory mucosa that lines most of the nasal cavity [24]. It consists of the olfactory epithelium, basal lamina, and lamina propria. The olfactory epithelium is thicker than the respiratory mucosa and is made up of bipolar olfactory receptor neurons (also referred to as olfactory receptor cells or olfactory sensory neurons), basal cells, supporting cells (sustentacular cells) and other cells such as the microvillar cells (Fig. 2) [25]. Each olfactory receptor neuron expresses a gene coding for only one type of olfactory receptor and can only detect one type of odorant molecule [26]. Through axonal targeting, the axons of the olfactory neurons that express the same kind of receptors aggregate in the same area of the olfactory bulb in structures called the olfactory glomeruli [27]. The “one neuron, one receptor” rule and axonal targeting allow odor discrimination (Fig. 1). Signals from olfactory receptor neurons are delivered to the olfactory glomeruli in layer II, or the glomerulus layer of the olfactory bulb [28].
Properties of olfactory receptor cells
In olfactory receptor neurons, signals are relayed via the G-protein alpha subunit (Gαolf). Proteins such as Gαolf and adenylyl cyclase III (located downstream of the pathway), are mainly distributed in the cilia of olfactory receptor neurons [22]. Patients with mutations in genes related to the cilia of the olfactory receptor neuron, such as Bardet-Biedl syndrome, can exhibit anosmia [29,30]. Olfactory neurons have a unique ability to regenerate throughout life [31]. The basal cells of the olfactory epithelium can be categorized into horizontal basal cells (HBCs) and globose basal cells (GBCs). HBCs function as stem cells, while GBCs play a role in the regeneration of the olfactory receptor neurons [32,33]. In aging, the rate of GBC proliferation into olfactory receptor neurons slows, resulting in delayed replacement of damaged olfactory neurons. Therefore, olfactory dysfunction may follow if damaged olfactory neurons are not substituted promptly [34].
The central pathways of olfaction
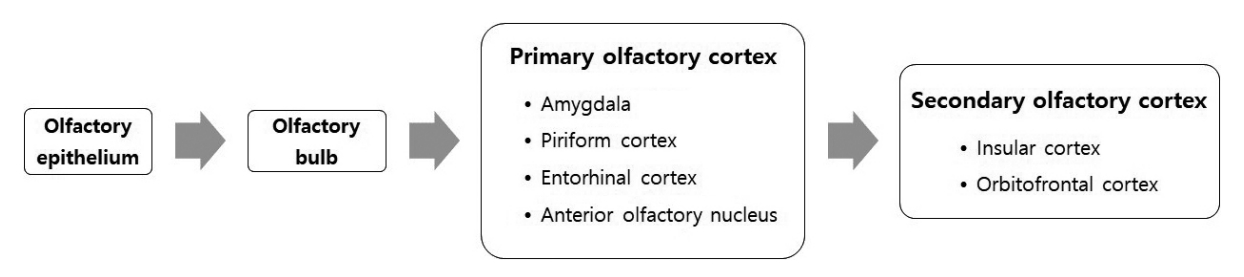
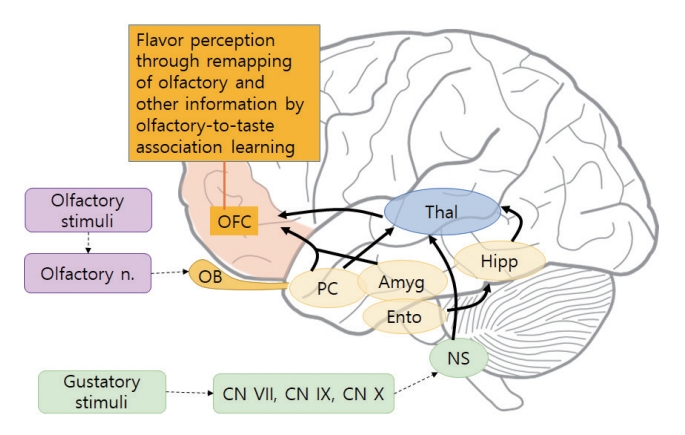
Olfactory receptor neurons form synapses with main olfactory bulb neurons, and mitral and tufted cells in the olfactory bulb project their axons to the primary olfactory cortex through the olfactory peduncle. From the olfactory peduncle, the axons then continue to the lateral olfactory tract, and thus the signals from the olfactory bulb are relayed to the primary olfactory cortex (anterior olfactory nucleus, piriform cortex, entorhinal cortex, and olfactory tubercle) (Fig. 3). The cortical networks that receive signals from the olfactory bulb commonly consist of multiple layers. Unlike the other senses, olfactory nerve fibers project to the primary olfactory cortex (amygdala, piriform cortex, anterior olfactory nucleus, and entorhinal cortex) without thalamic relay [35]. Thus, the olfactory system is a direct and rapidly responsive sense that quickly and subconsciously elicits emotions and/or memories. The orbitofrontal cortex, which consists of the secondary olfactory cortex, is responsible for combining taste and olfactory stimuli to form flavor, along with visual information [36].
Flavor
The orbitofrontal cortex consists of the secondary olfactory and gustatory cortex, combining visual and tactile information to form flavor [37]. In this manner, olfaction, taste, vision, and touch combine to produce flavor. The response provoked in neurons by olfactory stimuli is also combined with taste, which allows training by associative learning. Odor perception occurs both through the binding of odorants to the olfactory receptor neurons and the remapping of olfactory information in the orbitofrontal cortex with other associated information to perceive it with appropriate meaning. For example, tasting wine involves a process of olfactory-to-taste association in which the aroma and the taste combine in the orbitofrontal cortex to form flavor (Fig. 4).
OLFACTORY DYSFUNCTION AS A SYMPTOM OF NEUROLOGIC AND PSYCHIATRIC DISEASE
Gradual-onset olfactory dysfunction is a possible symptom of neurodegenerative diseases such as AD or PD [19]. Olfactory dysfunction is found in 90% of early-stage PD patients [38]. The olfactory bulb is one of the earliest affected regions in patients with PD. As PD progresses, pathology spreads from the olfactory bulb, anterior olfactory nucleus, and lower brainstem to other brain regions [39]. A hypothesis has suggested that environmental toxins that cannot move across the blood-brain barrier may induce inflammation in the olfactory mucosa and olfactory bulb, spreading to other brain regions [40]. The odor identification test in PD is considered one of the two-factor assessments for predicting the conversion risk of prodromal Parkinson’s patients [41].
In AD, neurofibrillary tangle formation and β-amyloid deposits have been observed in every layer of the olfactory bulb. The odor identification score of AD patients was significantly lower than that of normal controls, and this score worsened with the progression from minimal cognitive impairment to AD [42]. The odor identification test is also considered one of the 5-factor assessments to predict conversion from minimal cognitive impairment to AD within 3 years [41]. Thus, it has been suggested that declining olfactory function in the process of aging may be the result of early Alzheimer-type pathology in the olfactory system [43]. In addition, rapid olfactory decline during aging predicts dementia and gray matter volume loss in brain regions affected by AD [44]. Central nervous system demyelinating diseases, including multiple sclerosis, are also associated with olfactory loss [45], and patients with other neurological disorders, such as epilepsy, exhibit olfactory dysfunction [46]. Olfactory loss is noted as a common symptom of psychiatric conditions including schizophrenia, bipolar disorder, and major depressive disorder [47], and an increase in olfactory function is associated with a decline in depression severity [48]. Traumatic brain injury can also induce olfactory dysfunction and may indicate other neurologic complications [49]. In patients recovering from traumatic brain injury, neurogenesis and migration to the olfactory bulb from the subventricular region have been described previously [50]. As otorhinolaryngologists, we should consider the possibility of neurodegenerative or psychiatric diseases and collaborate with other specialists in this field when assessing patients with olfactory dysfunction.
TREATMENT OPTIONS FOR OLFACTORY DYSFUNCTION
The treatment options for olfactory dysfunction depend mainly on the etiology (e.g., trauma or sinonasal disease) and also involve correcting underlying metabolic or autoimmune conditions. The evidence for the use of local and systemic steroids, which are commonly prescribed for olfactory dysfunction, is limited. Intranasal sodium citrate may potentially improve olfactory outcomes in patients with PIOD [51]. Supplements such as zinc and α-lipoic acid have been studied, while in one randomized controlled trial, omega-3 fatty acids had a protective effect for patients undergoing endoscopic skull base surgery [52]. In a recent study, the use of platelet-rich plasma in the treatment has shown the potential to improve olfactory function in COVID-19–related smell loss [53]. Olfactory training is one of the few recommended treatment options for olfactory dysfunction, and combining other methods such as budesonide irrigation and omega-3 fatty acid supplementation may also be helpful [54,55].
The effect of olfactory training suggests the reversibility of olfactory dysfunction and plasticity of the olfactory system to some extent. After Hummel and colleagues reported the effects of olfactory training [56], many studies have investigated the possibility of olfactory training in improving olfactory function. Of note, the purity, concentration, and brand of odorants are not important, so patients can use anything with an odor to perform this training [57]. Olfactory training is one of the highly recommended treatment options in PIOD [20], and it has also been proven effective in a Korean cohort [58]. A systematic review and meta-analysis reported that olfactory training might be beneficial even for posttraumatic olfactory loss [59]. The mechanism of how olfactory training improves olfactory function has been investigated in several neuroimaging studies. Olfactory training increased the cortical thickness of several brain regions involved in olfactory processing, including the right inferior frontal gyrus, superior temporal gyrus, and entorhinal cortex [60]. Studies analyzing functional magnetic resonance imaging (MRI) in association with olfactory training have reported changes in connectivity within the visual cortex [61] and alterations in the connectivity networks [62], suggesting a reorganization of the neural associations. Studies have also demonstrated an increase in olfactory bulb volumes after olfactory training [63]. These studies suggest that improved olfaction consists of the reorganization of neural connectivity and possibly reflects structural changes in the olfactory system.
COVID-19 AND OLFACTORY DYSFUNCTION
Several mechanisms for how SARS-CoV-2 infection induces olfactory dysfunction have been suggested. Radiological imaging analysis examining changes in olfactory structures has reported that COVID-19 patients with olfactory loss exhibited opacification of the olfactory cleft, suggesting a conductive type of olfactory dysfunction [64]. Others noted that SARS-CoV-2 infection was associated with damaged olfactory epithelium [65,66], as well as down-regulation of olfactory receptors and the signaling components [67]. Furthermore, structural changes were also reported, including olfactory bulb atrophy [68,69]. In a longitudinal study comparing MRI before and after SARS-CoV-2 infection, those with a history of infection showed (1) a greater reduction in gray matter thickness in the orbitofrontal cortex, (2) more remarkable changes in markers signifying tissue damage in regions functionally related to the primary olfactory cortex, and (3) more significant reduction in global brain size [70]. Furthermore, these subjects also showed a greater decline in cognitive abilities compared to the control group. In another longitudinal cohort study, severe COVID-19 (based on the American Thoracic Society guidelines for community-acquired pneumonia) was associated with an increase in risk of longitudinal cognitive decline [71]. A study examining postmortem samples of COVID-19 patients identified multifocal microvascular injury in brain and olfactory bulb through MRI and histopathological examinations, but with no sign of viral infection in these samples [72]. However, another study on deceased patient samples suggested that sustentacular cells were the main target cell type in SARS-CoV-2 infection, rather than the olfactory receptor neurons [73]. Olfactory dysfunction due to SARS-CoV-2 infection seems to involve either the central or the peripheral olfactory system, or both. Considering that olfactory receptor neurons regenerate every 30 to 90 days, the mechanism may be different in each case. In comparison, mechanisms such as inflammatory cell recruitment and secretion of cytokines causing the loss of olfactory receptor neurons have been suggested for PIOD [74]; however, no studies have examined in depth the effect of these viral infections on the central nervous system. A study comparing MRI findings in PIOD and COVID-19-related anosmia showed a higher rate of abnormal shapes and greater signal intensity of the olfactory bulbs in COVID-19 patients [75]. Patients with smell and taste disorder related to COVID-19 were younger and scored higher on olfactory function tests, and a lower percentage of them had anosmia or ageusia than patients with PIOD [76]. As for the prognosis, approximately one-third of PIOD patients recover after 1 year [77]. In a meta-analysis, 95.7% of COVID-19 patients recovered their sense of smell at 180 days, while it was estimated that 5.6% of patients may have persistent olfactory and taste dysfunction [78]. While COVID-19 is considered endemic in many countries as of 2023, the sequelae of long-haul COVID-19 remain to be investigated.
CONCLUSION
As olfactory dysfunction receives greater public attention as one of the major symptoms of SARS-CoV-2 infection, we have realized the importance of olfaction in our daily lives. Humans have an olfactory system with complex pathways that allow us to perform as well or even better than some other mammals. The “one neuron, one receptor” rule and axonal targeting allow us to discriminate tens of thousands of odors, if not more. Olfactory nerve fibers project to the primary olfactory cortex without thalamic relay, which elicits immediate emotional and memory recall.
The orbitofrontal cortex is responsible for combining taste and olfactory stimuli to form flavor by associative learning. In addition to being indicatory of disease in the nasal cavity, olfactory dysfunction may also suggest neurodegenerative or psychiatric disease. Olfactory training is now considered an important tool for improving smell by reorganizing olfactory processing and network connectivity. COVID-19 related olfactory dysfunction may involve not only the peripheral part of the olfactory system, but also the central olfactory regions. Otorhinolaryngologists must have a basic understanding of the olfactory system and the pathophysiological mechanism related to the peripheral and central olfactory pathways to help patients when diagnosing and managing olfactory dysfunction.
HIGHLIGHTS
▪ Humans have complex olfactory pathways that allow us to perform as well as or even better than some other mammals.
▪ About one-fifth of the general population has olfactory dysfunction.
▪ Olfactory dysfunction is closely associated with neurodegenerative and psychiatric diseases.
▪ Sound localization performance improved after VR-based training in individuals with SSD and normal hearing.
▪ Olfactory training improves olfactory function, possibly through the reorganization of neural connectivity.
▪ Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) may cause olfactory dysfunction by affecting peripheral and central parts of the olfactory system.