Nasal Deformity Due to Tuberculous Chondritis
Article information
Abstract
Tuberculosis (TB) is a common disease worldwide. However, nasal TB is quite rare, and the diagnosis of nasal TB requires a high index of suspicion. The most common symptoms of this unusual presentation are nasal obstruction and nasal discharge. We present a case of nasal TB with involvement of the hard palate presenting with a chronically progressive nasal deformity and ulceration of the hard palate. A biopsy confirmed the diagnosis, and medication for TB was started and the lesions resolved. When a patient presents with chronic ulcerative lesions that do not respond to antibiotic treatment, TB should be included in the differential diagnosis. Biopsy of the lesion can aid in the confirmation of the diagnosis.
INTRODUCTION
Tuberculosis (TB) is a disease caused by Mycobacterium tuberculosis. The most commonly involved organ is the lung, and extrapulmonary TB accounts for only about 15% of all TB cases [1]. The overall incidence of TB has declined since the mid-20th century: however, there has been a recent resurgence, probably due to the emergence of resistant strains and an increase in the number of immunocompromised hosts [1,2].
Nasal TB was first reported in 1761 by Morgagni [3] who described the autopsy findings of a young man with ulceration of the soft palate, nasopharynx, and nose. In Butt's review of nasal TB in the 20th century, only 12 out of the 35 identified cases represented primary nasal TB [4]. The most common symptoms were nasal obstruction and nasal discharge. Less common symptoms included nasal discomfort, the presence of a mass, epistaxis, crusting, watering of the eyes, postnasal drip, recurrent polyps, and a nasal ulcer [4].
As nasal TB is quite rate, many clinicians have limited experience with the diagnosis. Nonetheless, nasal TB should be included in the differential diagnosis of chronic inflammatory lesions of the nose [2,4]. We present a case of nasal TB presenting as a nasal deformity with chronic ulceration of the hard palate.
CASE REPORT
A 57-year-old woman presented to the hospital for management of a nasal deformity. She had been treated for an abscess of the nasal cavity 15 years prior and had been managed with antibiotics intermittently without improvement. Since that time, her nose had become deformed. She also complained that she could not eat spicy food because of hard palate pain. She had no documented personal or family history of TB.
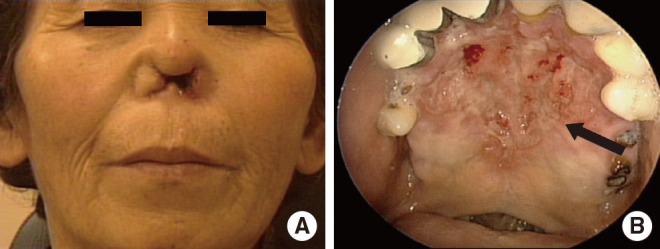
Her physical examination showed a defect of the cartilaginous portion of the nose with destruction of the nasal septum and cleft in the nasal alar area. There was also a yellowish discharge (Fig. 1A, B) and ulceration of the hard palate (Fig. 1C). Erosion of the epiglottis was observed on laryngoscopic examination. On admission, her body temperature was 36.2℃, blood pressure was 110/70 mmHg, pulse rate was 80/minute, and respiratory rate was 20/minute. The results of her laboratory tests were all within normal limits. Chest X-ray showed no evidence of pulmonary TB. A computed tomography scan of the head and neck showed a defect of the external nose and anterior cartilaginous nasal septum (Fig. 2).

Initial physical examination. The patient presented with a nasal deformity with inflammation (A, B) and a chronic ulcerative lesion of the hard palate (C, arrow).

Computed tomography findings. Perforation of the nasal septum of cartilaginous portion and defect of external nose.
A biopsy of the ulcerative lesion of the nasal septum and hard palate was performed. The pathology showed chronic granulomatous inflammation with caseous necrosis (Fig. 3B, arrow). A few acid-fast bacilli (AFB) were seen on Ziehl-Neelsen stain (Fig. 3B, arrow), and TB polymerase chain reaction (PCR) was positive. However, culture was negative for TB.

Histopathology of the nasal tissue. (A) Collections of epithelioid histiocytes forming granulomas and multinucleated giant cells against a necrotic background (H&E, ×100). (B) A few acid-fast bacilli were observed (Ziehl-Neelsen, ×1,000).
After one year of anti-TB therapy including isoniazid, rifampicin, ethambutol, and pyrazinamide, the wound healed and there was no discharge (Fig. 4) and the patient regained her ability to eat spicy food. The deformity, which was caused by inflammation, was unchanged. The patient has remained well without relapses for two years.
Follow-up physical examination. Following one year of treatment, the inflammation of the nasal deformity (A) and the chronic ulcerative lesion of the hard palate (B, arrow) both improved.
DISCUSSION
TB is still prevalent worldwide and constitutes a significant global health problem [5]. Approximately one third of the world's population is currently infected with TB and about 47% of infected people live in Southeast Asia [6]. Extrapulmonary TB accounts for about 15% of TB cases [1], and nasal TB chondritis is quite rare. In Butt's review of 35 cases of nasal TB, chondritis as found predominantly among women and in the elderly, and the most commonly affected site was the cartilaginous septum followed by the inferior turbinates [2,4]. The most common symptoms were nasal obstruction and nasal discharge. Less common symptoms included nasal discomfort, the presence of a mass, epistaxis, crusting, watering of the eyes, postnasal drip, recurrent polyps, and a nasal ulcer [4]. Our patient also had nasal discharge, ulceration and deformity of the nose, which is consistent with clinical descriptions in other studies.
The average duration of symptoms prior to diagnosis in Kim's study was six months [2]. In contrast, our patient had symptoms for 15 years, which is notably longer than in other reported cases.
The most probable routes of infection are mainly associated with secondary infection from pulmonary TB, with the infection spreading by contagious, hematogenous or lymphatic routes. In addition, dust or sneezing droplets from infected persons may introduce the organism into the nasal mucosa without first infecting the lungs [7], and direct inoculation by contaminated fingers has also been implicated [4].
Diagnosis of nasal TB requires a high index of suspicion. Radiological investigation may be helpful when TB of the head and neck is suspected. Histopathological examination is required for the diagnosis [8]. The first biopsy from our patient showed chronic inflammation only. We repeated the biopsy and took samples from the ulcerated nasal lesion, which revealed chronic granulomatous inflammation with caseous necrosis. Although isolation of M. tuberculosis from tissue culture is the definitive diagnosis, positive AFB staining or TB PCR of infected tissue can be also used as alternative diagnostic methods [9].
When granulomatous tissue proliferation, ulceration and reddish nodular hypertrophy are apparent, nasal TB should be suspected. The differential diagnosis should include infections which cases similar lesions, including viral (Herpes simplex), tuberculous (atypical TB, leprosy), bacterial (rhinoscleroma), treponemal (syphilis), fungal (mucormycosis, aspergillosis, blastomycosis, histoplasmosis, rhinosporidiosis), and parasitic (leishmaniasis) infection. Inflammatory disorders such as Wegener's granulomatosis, sarcoidosis, inhalation granuloma and natural killer-T cell lymphoma should also be considered [2,7].
Once the diagnosis of nasal TB has been established, conservative therapy with TB medications is the mainstay of treatment: surgical excision is usually not necessary [2,8]. The appropriate treatment of nasal TB is similar to that of systemic TB [9]. Any patients who have not been treated previously for TB should receive the internationally accepted first-line treatment regimen of isoniazid, rifampicin, pyrazinamide, and ethambutol [10]. The response to treatment is best assessed clinically [10], and the duration of treatment with the medication is usually 6-12 months for a cure [2,11].
TB has the potential to involve every organ, including the nasal cavity. When a patient presents with chronic inflammation of the nose that does not respond to antibiotic treatment, TB should be included in the differential diagnosis.
Notes
No potential conflict of interest relevant to this article was reported.