Comparison of Local Sclerotherapy With Lauromacrogol Versus Nasal Packing in the Treatment of Anterior Epistaxis
Article information
Abstract
Objectives
Epistaxis is one of the most common otorhinolaryngologic emergencies representing more than 12% of conditions managed at the Ear, Nose and Throat (ENT) Emergency Consulting Room of our Otorhinolaryngologic Unit each year. The elevated frequency of this pathology makes it necessary to adopt the most effective and least expensive therapeutic strategy available. The aim of this study was to compare the efficacy, costs and morbidity of nasal packing (NP), which is the mainstay of treatment for anterior epistaxis in our ENT Emergency Consulting Room versus submucosal infiltrations of lauromacrogol (LA).
Methods
A retrospective study was designed from August 2012 to April 2013 involving 53 patients suffering from anterior epistaxis. Anterior NP was used in 27 patients versus 26 patients undergoing 27 procedures performed with submucosal infiltrations of LA (or polidocanol). Outcomes for each treatment were evaluated. Patients in group 1 were treated with LA 400 injection next to the bleeding point: 0.5- to 1-mL single or multiple infiltrations with a 27-gauge needle. The whitening of the nasal mucosa around the bleeding point during infiltration was considered a marker of correct procedure in order to achieve the best results. Bilateral treatment was also performed at the same time. Patients in group 2 were treated with standard NP.
Results
Bleeding recurrence was higher in the NP group even if it was not statistically significant (P=0.2935). However, the LA infiltrations were better tolerated with lower morbidity and costs as compared to NP. No complications were observed in either group.
Conclusion
LA infiltrations were shown to be a viable alternative in anterior epistaxis treatment. They are safe, easy to use with good efficacy and have a low cost.
INTRODUCTION
Epistaxis is one of the most common otorhinolaryngologic emergencies representing more than 12% of conditions managed at Ear, Nose and Throat (ENT) Emergency Consulting Room (ECR) of our Otorhinolaryngologic Unit each year. It affects up to 60% of the population during their lifetime, with 6% requiring medical attention [1-5]. It is more common in the older population [2]; the greatest peaks in the overall incidence occur in individuals under 10 years of age and over 40 years of age [6].
The most common etiology is idiopathic [6]; in 80%–90% of cases, no precipitating causes can be identified [2,5]. Of the other identifiable causes of epistaxis, the most frequent are trauma, nasal neoplasm, iatrogenic or due to systemic factors (hypertension, coagulopathy, inflammatory conditions, infectious diseases, vessel wall fibrosis in the tunica media associated with ageing), use of drugs (anticoagulant, antiplatelet, nonsteroidal anti-inflammatory, nasal sprays) and congenital nasal septal abnormalities [2,6].
Epistaxis is classified as anterior or posterior on the basis of the primary bleeding site [7]. Anterior bleeds are the most common (80%–95%) [2,5] and occur from the anterior nasal area, also known as Kiesselbach’s plexus (or Little’s area or locus Valsalvae), which is anatomically formed by the anastomosis between the terminal branches of the external and internal carotid arteries.
The high incidence of epistaxis in the general population represents a significant healthcare cost and presents us with the opportunity of modifying the cost-benefit equation by adopting effective management strategies [8]. The aim of this study was to compare the efficacy, costs and morbidity of nasal packing (NP), which is the mainstay of treatment for anterior epistaxis in our ENT ECR, versus submucosal infiltrations of lauromacrogol (LA).
Lauromacrogol (or polidocanol) is a polyethylene glycol monododecyl ether, which has a selective effect on the venous endothelium, leading to a secondary thrombosis without necrosis in the surrounding tissue, providing this is healthy and well irrigated. At the end of the process, the obliterated vein is replaced with connective fibrous tissue. As it is a stable compound at room temperature and has low viscosity, its administration is very simple and efficient in intralumen, submucosal infiltrations. It is commercially available as Aethoxysklerol (Kreussel Pharma, Chemische Fabrik Kreussler & Co., Wiesbaden, Germany) and comes in boxes containing five 2-mL vials. We use vials of 1% which contain 20 mg of LA 400. Vials of 0.25%, 0.5%, 2%, and 3% are also available, with a total amount of LA of 5, 10, 40, and 60 mg, respectively.
Fifty-three patients suffering from anterior epistaxis were studied from August 2012 to April 2013. Anterior NP was applied in 27 patients versus 26 patients undergoing 27 procedures using submucosal infiltrations of LA. In both groups, efficacy, tolerance, complications and costs of treatment were analyzed.
MATERIALS AND METHODS
A retrospective study was designed involving patients with an anterior bleed from Kiesselbach’s plexus (which had not been resolved with the common method of applying pressure to this area) diagnosed and treated at the ENT ECR of our Otorhinolaryngologic Clinic from August 2012 to April 2013.
In order to avoid any bias, related to the choice of the treatment, only cases treated by 2 operators were selected. During the period of the study, despite the severity of the case, it was found that one operator performed only submucosal infiltrations of LA while the other performed only NP.
Patients eligible for the study were retrospectively divided into 2 groups. The patients in group 1 (LA group) were those treated with submucosal infiltration of LA by one operator while the patients in group 2 (NP group) were those undergoing NP performed by a second operator.
Admission criteria: Only patients with anterior and localizable epistaxis in Kiesselbach’s plexus were enrolled. Exclusion criteria: (1) secondary epistaxis (posttraumatic, postoperative, tumoral); (2) age less than 18 years; (3) pregnancy; (4) major systemic disease; (5) hereditary hemorrhagic telangiectasia (HHT); (6) lack of data in patient’s chart.
Epistaxis related to pharmacological therapy (anticoagulant) or to hypertension was not excluded.
In both treatments, the nasal cavity affected was first treated with cotton soaked with a few drops of a solution of lidocaine hydrochloride monohydrate 5.3 g and naphazoline nitrate 0.020 g ×100 mL (Xylocaine 5%, Astra Zeneca, Rueil-Malmaison, France) for a few minutes. This was used to obtain local anesthesia and nasal mucosae decongestion in order to reduce the bleeding and to better visualize the bleeding site. When necessary, a nasal endoscopy was also performed to exclude posterior bleeding and to obtain a better view of the anterior nasal mucosae.
The LA injection technique: 0.5- to 1-mL single or multiple submucosal infiltrations next to the bleeding point using a 27-gauge needle. Submucosal infiltration instead of subpericondrial infiltration was preferred in order to achieve a better outcome (the venous endothelium is located in the submucosal region) and to avoid septal cartilage necrosis. The whitening of the nasal mucosa around the bleeding point during infiltration was considered as a marker of correct procedure in order to achieve the best results. In patients with bilateral anterior epistaxis bilateral treatment was also performed at the same time. When there was persistence of bleeding from the site of the injection, a smooth NP with Gelita-Spon (Absorbable Gelatin Sponge, Gelita Medical, Amsterdam, The Netherlands) was carried out.
Infiltrations can be repeated when there is persistence of an exophytic septal vessel, even if asymptomatic, or in the case of persistence of bleeding.
Nasal packing: performed with short 4.5 cm or long 8 cm Merocel standard nasal dressing (Medtronic Xomed Inc., Jacksonville, FL USA). In some cases Merocel NP was used in combination with hyaluronic acid gauze pads.
No prophylactic systemic antibiotics were systematically prescribed in either group of patients. The patients were checked after 72 hours by the resident on duty in order to remove the NP or to evaluate the short-term results of the infiltration. After this follow-up, the patients were asked (by means of a telephone interview) to report any recurrence of epistaxis (and how it was treated) and any possible complication occurring during the first month after treatment, and to complete a questionnaire regarding treatment morbidity. Bleeding after thirty days was no longer considered as a recurrence.
The following were evaluated:
(1) the efficacy of the treatment after 3 days and after 1 month
(2) the treatment morbidity using a specific questionnaire: (i) with a numeric rating scale (NRS-11) which is an 11-point scale for self-reported pain during the execution of the treatment (ii) with a numeric rating scale from 0 to 5 to evaluate the most frequent symptoms during the first 72 hours after treatment (nasal congestion, epiphora, pain or headache, other).
(3) complications arising in the first month after the procedure
(4) cost of each procedure (excluding costs common to both)
Statistical analysis was carried out using SAS ver. 9.3. (SAS Inc., Cary, NC, USA). The Fisher exact test and Wilcoxon rank sum test (Mann-Whitney U-test) were used to compare the results.
This study was approved by our Institution Review Board (protocol number: 1585/2014).
RESULTS
Lauromacrogol (LA group)
Twenty-seven procedures using submucosal infiltration of LA were performed on 26 patients eligible for the study; one of these patients had a bilateral infiltration at the same time due to bilateral epistaxis.
There were 16 males and 10 females (male/female ratio, 1.6/1) and the mean age was 63±21 years ranging from 18 to 88 years, with a median value of 66 years.
The mean number of injections was 1.89 with a mean use of LA of 0.68 mL per procedure. In the majority of cases (66.66%), after treatment, the nasal cavity was packed with resorbable material Gelita-Spon (Absorbable Gelatin Sponge, Gelita Medical, Amsterdam, The Netherlands) positioned only over the bleeding site: in the remaining cases there was no need to position any resorbable packing. This material was used to avoid any possible bleeding from the injection site during the first hours after the procedure and to permit the safe return home of the patient after discharge, especially for the older patients if under anticoagulant therapy.
Three patients were excluded from our series because the nasal cavity was packed with a short Merocel for 48 hours after infiltration. The use of such NP in these cases was justified by elevated blood pressure or anticoagulant therapy associated with advanced age (all over 84 years of age). In these patients, there was a high risk of a recurrence of bleeding which could represent a serious social and management problem.
The frequency of hypertension in the group selected was 61.54%, and 30.77% of the patients were under warfarin or aspirin therapy.
In 3 cases (11.11%), there was a recurrence of epistaxis which occurred after 3–13 days (mean, 9 days); it was treated with anterior NP. All patients suffered from uncontrolled hypertension, and 1 patient was under aspirin treatment.
In 2 of these cases, after the removal of the NP, there were no more bleeding episodes. In the last case, the patient underwent bipolar cautery one month after the first episode.
The 3-day follow-up showed some minor self-contained bleeding in 3 cases (11.11%) and some crust formation in 3 cases (11.11%).
Nasal packing (NP group)
Twenty-seven treatments with NP were performed on 27 patients eligible for the study. There were 14 males and 13 females (male/female ratio 1.08/1) and the mean age was 75±18 years ranging from 20 to 96 years, with a median value of 79 years.
In 8 cases, due to the presence of a septal spur, standard packing with short or long Merocel was associated with the use of hyaluronic acid gauze pads; this helped to achieve a more efficient control of the bleeding in these cases.
NP was always removed approximately 72 hours after treatment in order to reduce patient’s discomfort and to avoid the use of antibiotics (normally advisable for longer packing).
The prevalence of hypertension in the group selected was 81.48%, and 59.26% of patients were under warfarin or aspirin therapy.
Seven patients had a recurrence of epistaxis (25.93%): all patients suffered from uncontrolled hypertension, and 4 patients were under anticoagulant treatment. One patient returned to our ECR 12 hours after treatment for persistence of the epistaxis, and a short Merocel was added to the two already present. In 3 cases, it occurred just after the programmed nasal dressing removal and required new NP. Three patients had a recurrence of epistaxis from the same source of bleeding 8, 17, and 30 days, respectively, after the first episode and were treated with NP. Two patients in this group underwent bipolar cauterization and one treatment with LA while, in the last 4 cases, there was no need for other treatment.
Comparison
The results for each procedure are compared in Table 1. Bleeding recurrence was higher in the NP group even if the value was not statistically significant (P=0.2935 using Fisher exact test) also when considering only patients using anticoagulant therapy (P=0.6206) or those not using anticoagulant therapy (P=0.3386). Eleven patients complained of pain during execution of the procedure in the LA group versus 22 in the NP group; the highest reported pain value in the LA group was 3 versus 9 in the NP group. The mean pain value was statistically higher in the NP group: P<0.0001 using the Wilcoxon rank sum test (Mann-Whitney U-test). The mean cost for each procedure was lower in the LA group (4.42 Euro [EUR] vs. 7.36 EUR for each procedure).

Results for each procedure
Comparison of the morbidity in the first 72 hours after each treatment shows significantly higher discomfort in the NP group (Table 2). This was statistically significant when compared with the morbidity in the LA group considering nasal congestion (P<0.0001), epiphora (P<0.0001) or, in particular, headache/pain (P<0.0001).
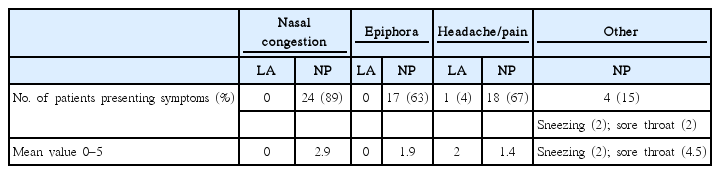
Comparison of morbidity between the two procedures
DISCUSSION
The elevated healthcare costs due to the high frequency of epistaxis, which is one of the most common otorhinolaryngologic emergencies, require the adoption of the most effective and least expensive therapeutic strategy to reduce inpatient stay, surgical rates and transfusion rates [8]. Another aspect which should be considered is the discomfort and pain caused by each of the several kinds of treatments proposed for epistaxis [4]. For these reasons, it is also important to choose the method best accepted by the patients which should have 3 characteristics: minimal discomfort, cost effectiveness and low level of recurrence [4].
The basic approach to any case of epistaxis consists of three steps: identification of the bleeding site, stopping the bleeding and identification and treatment of the underlying cause, if any [6].
Submucosal infiltration of LA is a well-established treatment which has already proven its effectiveness in HHT or Rendu-Osler-Weber disease [9] being the epistaxis the most frequent clinical manifestation in HHT. Epistaxis results from rupture of the telangiectases present in the nasal mucosa, leading when severe, to recurrent visits to emergency units, periods in the hospital and transfusions, thereby, endangering the physical integrity of patients and reducing their quality of life [9]. On the basis of the data collected by Morais et al. [9] and considering our experience in the treatment of HHT with LA injection in the last 7 years, it was also decided to try this technique on patients with anterior epistaxis. This type of procedure is simple and can easily be performed as an office procedure with local anesthesia. Preparing the nose with an anesthetic and a decongestant helps to find the site of the bleeding and causes the patient less discomfort [1].
For many years, the mainstay of treatment for anterior epistaxis was NP [6]: this technique is still considered useful when it is not possible to identify the bleeding point, even with a nasal endoscope [5]. In the majority of patients, when the bleeding point in the anterior part of the nose is evident, epistaxis can be better controlled with direct cautery [8] without resorting to NP [10]. Silver nitrate cautery is also an effective treatment and can prevent recurrence [11]. These types of treatment can avoid the morbidities associated with NP, including pain, necrosis of the nasal ala, hypoxia [6], toxic shock syndrome, septal hematoma and abscess, Eustachian tube dysfunction, acute sinusitis, epiphora, hearing loss, dysphagia, displacement of the packing into the oropharynx resulting in acute airway obstruction, aspiration and respiratory arrest [2].
The data collected by our study cannot demonstrate a statistically significant difference in outcome between the 2 arms; however, for the patients in the LA group, tolerance was better during treatment and also during the following days. Only 1 patient referred pain for a few days after the injection, no patient presented epiphora or nasal congestion and the mean pain value during the execution of the treatment on a numeric rating scale (NRS-11) was clearly lower than the NP group (0.6 vs. 3.2). Moreover, in the majority of cases in the LA group, the discomfort of NP removal and bleeding risk after NP removal were eliminated. No major complications (nasal perforation, septal abscesses, etc.) occurred in either group after the first follow-up and no complications were reported during the telephone interviews. The cost analysis showed that the LA treatment was cheaper than NP with a medium cost of 4.42 EUR versus 7.36 EUR. This is reinforced by the fact that patients with NP absolutely require a second visit to remove the Merocel or Hyaluronic acid gauze pads leading to additional cost. On the contrary, there is no need for a second visit after LA injection unless there is a recurrence of epistaxis. Our results confirmed those obtained of Morais et al. [9] regarding the treatment of HHT in terms of both efficacy and complications; in their series, only 1 case of septal perforation was reported in 300 procedures.
For the above-mentioned reasons, this technique represents a viable alternative to the other methods proposed for anterior epistaxis treatment. It fully meets the requirements for the ideal treatment of epistaxis: good efficacy, well tolerated by the patient and low cost. Moreover, the use of expensive devices requiring a specific environment, such as in the case of bipolar diathermy despite its proven effectiveness, is unnecessary [2,12, 13]. In our ECR, for example, cauterization can be performed only in the operating room leading to higher costs, loss of time and resources, and the need to hospitalize the patient.
A possible alternative to NP and the other surgical techniques available at our institution is the use of Floseal (Baxter Healthcare Corp., Zurich, Switzerland). Floseal, a novel hemostatic composed of collagen-derived particles and topical bovine-derived thrombin, is a better tolerated, safe and easy alternative to NP in patients with acute anterior epistaxis [14]; however, costs are higher with Floseal [6].
The introduction of rigid nasal endoscopes for the diagnosis and therapy of sinonasal pathologies also permits using them for the treatment of epistaxis because their usefulness in identifying the bleeding point [1]. Endoscopic exploration of the nasal cavity permits more precise identification and treatment of the area to be infiltrated, and excludes or reveals other potential points of bleeding. With the help of endoscopes, it is also possible to treat more posterior sources of bleeding with the LA infiltration technique.
In conclusion, LA infiltration was demonstrated to be a viable alternative in anterior epistaxis treatment. It is safe, easy to use, and has good efficacy and low costs.
Notes
No potential conflict of interest relevant to this article was reported.
Acknowledgements
We would like to thank Elisa Carretta for providing the statistical analysis.