Effect of Chronic Rhinosinusitis With or Without Nasal Polyp on Quality of Life in South Korea: 5th Korea National Health and Nutrition Examination Survey Korean
Article information
Abstract
Objectives
This is the first study of its kind to investigate the relationship between chronic rhinosinusitis (CRS) with or without nasal polyps (NP) and health-related quality of life (HRQoL) in the general adult Korean population. We sought to evaluate the association after adjustment for confounding factors. We also evaluated HRQoL according to presence of NP in CRS patients.
Methods
In this cross-sectional study we used nationally representative samples from the 5th Korea National Health and Nutrition Examination Survey (2010–2012). A total of 17,490 participants were included in the study, of which 613 were diagnosed with CRS. Univariate analysis was conducted on healthy versus CRS groups, segregated by gender with weighted prevalence of demographic characteristics, socioeconomic status, and comorbid diseases. Subanalysis was carried out to evaluate the relationship between CRS with or without NP and HRQoL using EuroQol 5-dimension (EQ-5D) and visual analog scale (EQ-VAS). The odds ratios for EQ-5D were estimated by multiple logistic regression analyses with confounder adjustment.
Results
Weighted prevalence of CRS of adult male was found to be 3.7% and CRS with nasal polyps (CRSwNP) 0.5%, while female CRS was 3.3% and CRSwNP 0.3%. There was no significant difference between the groups (P#x0003d;0.332). The scores for female, EQ-5D index (P for trend<0.001) and EQ-VAS (P for trend=0.002) showed decreasing trend from healthy participants to CRS without nasal polyps (CRSsNP) and from CRSsNp to CRSwNP. After adjusting for demographic characteristics, socioeconomic status, and comorbid diseases, EQ-5D scores; EQ-5D index (P<0.001) and EQ-VAS (P<0.001) exhibited poorer HRQoL compared to healthy participants, exclusively within the female group.
Conclusion
These data suggest that female patients with CRS are at higher risk of poor HRQoL. In addition, HRQoL of female CRSwNP was lower compared to those of CRSsNP and healthy participants.
INTRODUCTION
Chronic rhinosinusitis (CRS) is a disease characterized by mucosal inflammation affecting the nasal cavity and paranasal sinuses. The most common symptoms of patients presenting with CRS include nasal congestion, nasal discharge fatigue, headache, hyposmia or anosmia, and facial pain. Data from the National Health Interview Survey of the United States reported CRS to be the second most prevalent chronic health condition, affecting 12.5%–16.0% of the US population [1-3]. In Europe, the European multicenter study on CRS found a prevalence of approximately 10.9% [4]. The prevalence of CRS in the Korean population is currently 6.95% [5]. Over the past 2 decades the focus of research has shifted from diagnosis and symptoms, to evaluation of a patient’s quality of life (QoL) [6] or more specifically, health-related QoL (HRQoL). The symptoms of CRS can be debilitating and can considerably affect HRQoL [7]. Informative assessment of QoL for CRS patients is of medical, social and economic importance. The presence of nasal polyps (NP) is positively correlated with CRS and considered a subgroup of CRS [8]; however, there have been no reports published that evaluate the association between CRS with NP (CRSwNP) or without NP (CRSsNP) and HRQoL at the population level. Moreover, no data currently exist describing this association between CRS and HRQoL within the general Korean population, specifically. Therefore, in this study we aimed to reveal the interaction between CRS and HRQoL using data from the Fifth Korea National Health and Nutrition Examination Survey (KNHANES), together with a subanalysis of CRSwNP or CRSsNP.
MATERIALS AND METHODS
Study population
This study was based on data acquired from the KNHANES V (2010–2012), a survey conducted by the Korea Centers for Disease Control. The protocol was approved by the Institutional Review Board at the Korea Centers for Disease Control and Prevention (2010-02CON-21-C, 2011-02CON-06-C, 2012-01EXP-01-2C), and all individuals signed informed consent forms. KNHANES V adopted the stratified multistage cluster random sampling, designed with a rolling-survey sampling method. This method allows samples to be collected that are representative of the general population and are independent and homogeneous. Between 2010–2012 otorhinolaryngologic survey participation totaled 23,621 individuals. From these participants we excluded those who were younger than 19 years (n=5,555) because of QoL evaluations were not performed under 19 years in KNHANES, and those who did not provide complete answers to questions regarding sinus symptoms, HRQoL, sociodemographics or comorbid diseases (n=576). Thus, a final total of 17,490 participants were identified as eligible for our study.
Demographic characteristics
Questionnaires were used by physicians or interviewers to collect subject information, in person. Age was divided into 7 subgroups by decade. Body mass index (BMI) was calculated as the individual’s weight in kilograms divided by the square of their height in meters. BMI and sleep time were compared by their mean values. Cigarette smokers were defined as those currently using tobacco or those who had smoked more than 100 cigarettes during their lifetime. The amount of alcohol consumed (in grams per day) was calculated by the average quantity and frequency of alcohol consumption. Participants who drank more than 30 g/day were classified as heavy drinkers [9]. Subjects who participated in moderate physical activity at least 5 days per week for more than 30 minutes each day and/or strenuous physical activity for more than 20 minutes per session at least 3 days per week were classified into the regular exercise group [10]. Residency was divided into urban and rural areas according to the official home address of the subjects. The ‘low income’ group was identified as those correspondents within the lowest quartile of household income. Education level was considered “high” if the participant completed education beyond middle school (higher than ninth grade). Marital status was divided into single or married. Comorbid diseases, such as allergic rhinitis, atopic dermatitis and asthma (physician determined diagnosis), were self-reported on the questionnaires.
Rhinologic symptoms and physical examination
Physicians evaluated rhinologic symptoms based on details obtained from the questionnaire. These included rhinitis, such as rhinorrhea, sneezing, itching sensation of nose, and indicating sinusitis, such as anterior/posterior nasal drip, nasal obstruction, facial pain, anosmia, or hyposmia. In addition, otolaryngologists examined all subjects’ nasal cavities using a 4-mm, 0° nasal endoscope to confirm symptoms and also reported on the presence of NP.
Diagnosis of CRS
The European Position Paper on Rhinosinusitis and Nasal Polyps (EPOS) provides guidelines for conducting epidemiological studies of CRS [8]. According to EPOS, epidemiological studies on CRS are based on specific self-reported symptoms. CRSwNP or CRSsNP is defined as the presence of two or more symptoms, one of which should be either nasal blockage/obstruction/congestion or nasal discharge (anterior/posterior nasal drip): ±facial pain/pressure; ±reduction or loss of smell; for >12 weeks [8]. A precise clinical diagnosis of CRS requires radiological imaging that includes computed tomography [8], which is not feasible in population-based studies. Therefore, in this study it was not possible to apply a definitive clinical diagnosis despite specific, self-reported symptoms. The otolaryngologists examined all participants with nasal endoscope after shrinking nasal mucosa to determine NP presence or absence.
EuroQol 5-dimension (EQ-5D)
EQ-5D is commonly used for determining HRQoL in patients and is considered an effective tool for evaluating the impact of CRS on overall patient health and health burden [11,12]. Importantly, EQ-5D has demonstrated significant associations with chronic rhinosinusitis outcome instruments, including the Chronic Sinusitis Survey and SinoNasal Outcomes Test-22 [12]. EQ-5D records information along 5 dimensions (i.e., mobility, self-care, usual activities, pain/discomfort, and anxiety/depression). For each dimension, participants choose one of 3 levels of severity (1, no problem; 2, some/moderate problems; 3, severe/extreme problems). Each dimension was divided as previously described [13]. Each dimension is weighted and summarized as an index-based score or ‘EQ-5D index’ [14]. EQ-5D index was conducted by Korea Centers for Disease Control in 2007. This method also includes a visual analog scale (VAS), called EQ-VAS, which records a patient’s “Health Today” as a score between 0 and 100.
Statistical analysis
Statistical analyses were performed using the SAS ver. 9.3 (SAS Institute., Cary, NC, USA). We measured the mean±SE or the proportion (SE). To determine the differences in general characteristics between CRSwNP or CRSsNP and healthy participants, continuous variables were tested with t-test using SURVEYREG procedure while categorical variables were tested with Rao-Scott chi-square test using SURVEYFREQ procedures. The weighted prevalence of CRSwNP or CRSsNP was calculated for the Korean population after being adjusted for strata and clustering at the primary sampling unit level. By multiple logistic regression analysis with SURVEYLOGISTIC, we tested the association between CRS patients and EQ-5D including EQ-5D VAS, while adjusting for confounding factors. Model 1 included an adjustment for demographic characteristics; age, sex, BMI, smoking status, alcohol use, and exercise status. Model 2 adjusted for socioeconomic status additionally; region of residence, income, education and marital status. In addition, Model 3, we adjusted for comorbid diseases; allergic rhinitis, asthma and atopic dermatitis. A P-value of <0.05 was considered to indicate statistical significance.
RESULTS
General characteristics
A total of 17,490 participants were included in the study (Table 1), of which 613 were diagnosed with CRS. By univariate analysis, prevalence of CRS was higher in younger participants (male, P#x0003d;0.041; female, P#x0003d;0.003), higher levels of education (female, P#x0003d;0.036), pain/discomfort dimension of EQ-5D (female, P<0.012), anxiety/depression dimension of EQ-5D (female, P<0.001), EQ-5D index (female, P#x0003d;0.003), EQ-5D VAS (female, P<0.001), allergic rhinitis (male, P<0.001; female, P<0.001) and asthma (female, P#x0003d;0.011). Females demonstrated a tendency towards a lower HRQoL by univariate analysis.
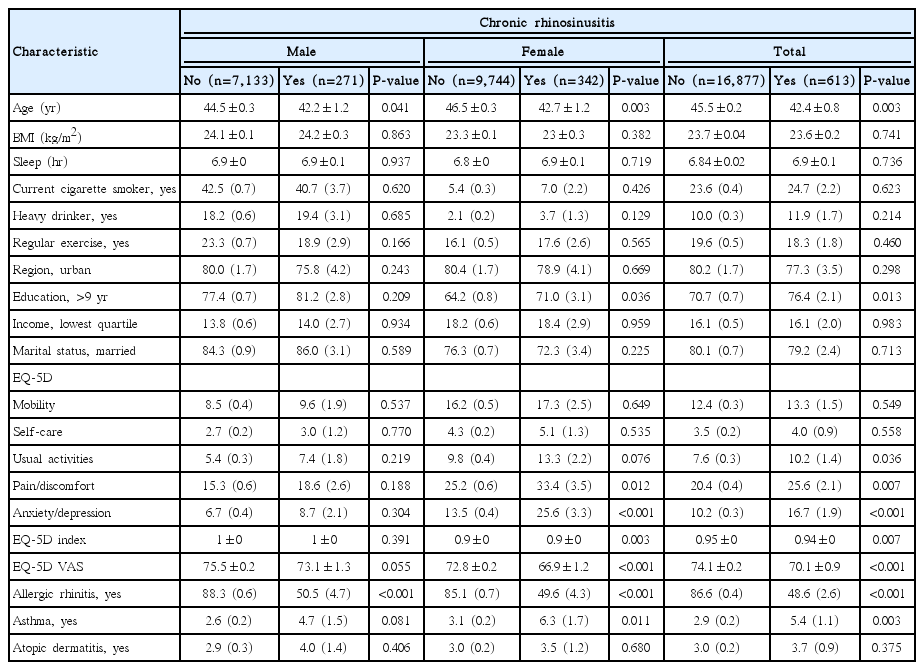
General characteristics of the total study population
Gender differences in prevalence of CRSwNP or CRSsNP
The prevalence of CRSwNP and CRSsNP, stratified by age and gender among the KNHANES 2010–2012 population aged ≥19 years, is presented in Fig. 1. The overall weighted prevalence of CRS in Korean adults was found to be 3.86%. The weighted prevalence of CRSwNP/CRSsNP for males was 3.7%/0.4% compared to 3.3%/0.3% for females. Males demonstrated a greater prevalence of CRS compared to females, other than in the age group 19 to 29 years. The age group 19 to 29 years showed the highest prevalence of CRS, but lowest NP prevalence in both genders. The prevalence of CRS between gender groups showed no significant difference (P#x0003d;0.332).
The prevalence of chronic rhinosinusitis (CRS) and CRS with nasal polyps stratified by age and gender. M, male; F, female; T, total; CRSsNP, CRS without nasal polyps; CRSwNP, CRS with nasal polyps.
Differences in HRQoL among healthy, CRSwNP, and CRSsNP subjects
To evaluate HRQoL differences among the healthy, CRSwNP and CRSsNP groups, we analyzed data using the ED-5D index score and ED-VAS score. Total participants trend from healthy to CRSsNP, CRSsNP to CRSwNP showed decreased in both EQ-5D index (P for trend=0.027) and EQ-VAS (P for trend <0.001). But there were some gender differences in scores. From healthy participants toward CRSsNP and CRSwNP, EQ-5D index (P for trend<0.001) and EQ-VAS (P for trend=0.002) scores decreased in female (Figs. 2, 3). But, male showed a decreasing scores trend only in EQ-VAS (P for trend=0.03), and observed lesser gap (Figs. 2, 3).
EuroQol 5-dimension (EQ-5D) index score according to participant group. CRSsNP, CRS without nasal polyps; CRSwNP, CRS with nasal polyps. Total, P for trend=0.027; male, P for trend=0.387; female, P for trend=0.002.

EuroQol visual analog scale (EQ-VAS) score according to participant group. CRSsNP, CRS without nasal polyps; CRSwNP, CRS with nasal polyps. Total, P for trend<0.001; male; P for trend=0.03; female, P for trend<0.001.
Multiple logistic regression analysis with confounder adjustment
A multiple logistic regression analysis describing the relationship between CRS and EQ-5D is presented in Table 2. Results are presented by EQ-5D QoL dimension, EQ-5D index score and EQ-VAS score. Using model 1 and adjusting for demographic characteristics, we identified several categories with significant differences in the CRS participants, including mobility, usual activities, pain/discomfort, and anxiety/depression (odds ratio [95% confidence interval]: 1.49 [1.121–1.982], 1.878 [1.344–2.625], 1.594 [1.262–2.013], and 1.986 [1.507–2.618]), also CRS participants demonstrated a lower EQ-5D index score (P<0.001) and EQ-VAS score (P<0.001), which correlated with a worse HRQoL. Data analyzed using model 2 (OR [95% CI]: 1.581 [1.148–2.177], 1.863 [1.302–2.043], 1.587 [1.233–2.043], and 2.096 [1.555–2.825]) and model 3 (OR [95% CI]: 1.571 [1.127–2.189], 1.823 [1.275–2.608], 1.53 [1.185–1.976], and 2.121 [1.563–2.877]), which adjusted for socioeconomic status and comorbid diseases, additionally, paralleled that seen with model 1. However, in analysis performed according to gender difference, female CRS patients result showed significant related with a worse HRQoL on the other hand, male showed lesser relationship (Table 3). Anxiety/depression domain of female, odds ratio was increased even after adjusting confounding factors additionally. Within the male population, only “usual activities” of EQ-5D, when using model 2 and EQ-VAS demonstrated any significant correlation.
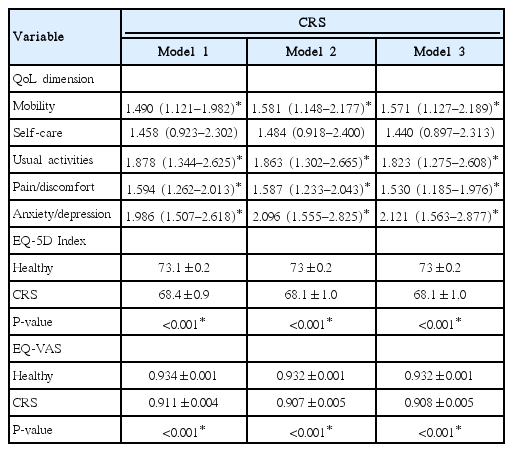
Relationship between CRS and EQ-5D using the multiple logistic regression
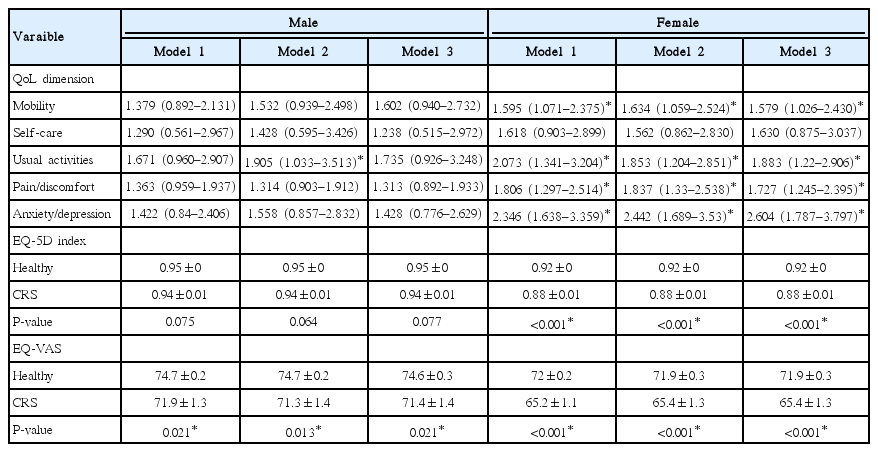
Gender differences between CRS and EQ-5D using the multiple logistic regression analysis
DISCUSSION
Our study was designed to assess the association between CRS and participant’s HRQoL using EQ-5D. We subjected adult participants to a thorough physical examination and solicited HRQoL answers to a detailed questionnaire.
Many confounding factors affect the severity of symptoms of CRS. One of the most important intrinsic factors is gender [15,16]. Several publications report that female patients with CRS claim to experience more severe symptoms compared to males [16,17], although contradictory data have also been reported [18]. This difference in gender experience of QoL was addressed by Mendolia-Loffredo et al. [19]. In their paper they explain gender differences in QoL are influenced by an increased prevalence of acetylsalicylic acid intolerance and depression in females. Moreover, Srivastava et al. [20] reported that sleep quality is significantly impacted for females with fungal CRS compared to male patients. For this reason we divided CRS patients by gender and evaluated other confounding factors that could affect a patient’s impression of symptom severity, including demographics, socioeconomic status, and comorbid diseases. Three distinct models were generated to individually adjust for these confounding factors when determining the effect of CRS on HRQoL. Presence of septal deviation was reported in KNHNES study, but not about severity and their effect on nasal passage. Including ambiguous factors can result in decreasing statistical power. So, we excluded deviated septum factor. NP cause nasal symptoms [21-24] and their effect on QoL have been described in several reports [21,25]. Also, It has been well documented that CRSwNP exhibit more extensive disease compared to CRSsNP. But there were no reports considering gender difference. In our study, we found no differences in EQ-5D index scores in males. The prevalence of Healthy, CRSsNP and CRSWNP in patients demonstrated a nonsignificant trend in the male group; however, females demonstrated lower scores in CRSwNP than CRSsNP participants. EQ-VAS score was found to be lower in CRSwNP than CRSsNP for both gender groups. These results suggest that CRSwNP is correlated with a worse HRQoL, comparatively for female patients. Collins et al. [26] hypothesize that aetiology of NP in men were related to exposure to occupational dusts and chemicals, while female were more associated with asthma, allergic rhinitis, and food allergies. We supposed that these aetiological differences can influence gender differences.
However, the severity of symptoms does not necessarily reflect the severity of disease and confounding environmental factors may affect the patient’s perception of symptom severity [19]. Thus, we assessed EQ-5D results and adjusted for potential confounding factors to achieve a more accurate evaluation of HRQoL in patients with CRS. Our results identify significant gender differences in the association between CRS and EQ-5D. For females, even after adjusting for potential confounding factors the association remained significant. Especially, the anxiety/depression domain of female was the highest odds ratio. Moreover, odds ratio was increased even after adjusting confounding factors additionally. Alternatively, male CRS patients demonstrated little association with EQ-5D, except for a single QoL dimension in model 2 and EQ-VAS. Thus, our study indicates that female patients with CRS appear to be at a higher risk for poor HRQoL than male patients. Furthermore, CRSwNP patients also expressed a reduced HRQoL, and this decline appeared more prominent in the female population.
There were several limitations to our study. First, it was of a cross-sectional design, which made it impossible to determine causative relationships. Second, diagnoses were self-reported and the study was subject to response bias with regard to several of the parameters. Third, because of small population of CRSsNP, authors do not analyze HRQoL between 3 groups. Notwithstanding the above-mentioned limitations, to our knowledge, this was the first population-based study to assess the relationship between CRS with or without NP and HRQoL in the general Korean population.
Our study identified female patients with CRS and CRSwNP as being at high risk for poor HRQoL. Moreover, anxiety and depression were strongly correlated with poor HRQoL in female. Thus, more attention should be paid to the psychological status of female CRS patients.
Notes
No potential conflict of interest relevant to this article was reported.