Results of Air Caloric and Other Vestibular Tests in Patients with Chronic Otitis Media
Article information
Abstract
Objectives
Air caloric results are supposed to be influenced by anatomic changes of the middle ear. The aims of our study were to evaluate the incidence and characteristics of abnormal air caloric results in patients with unilateral chronic otitis media and without any history of vertigo, and to compare caloric results with there of other vestibular function tests (VFTs).
Methods
Twenty five patients with unilateral chronic otitis media (COM) who were scheduled for surgery underwent VFTs preoperatively. Hearing was assessed using pure-tone audiometry and vestibular function was assessed using a set of VFTs: air caloric, head-shaking nystagmus (HSN), vibration-induced nystagmus (VIN), and subjective visual vertical (SVV) tests.
Results
Six patients (24%) showed pathologic canal paresis (CP) on COM-sided ears. Two patients showed pathologic CP on the contralateral side. However, both of the two showed inverted nystagmus to warm air stimulation on the COM-side and hyperactive nystagmus to cold air stimulation on the COM-side, which means that the COM-sided ear was stimulated too much. There was pathologic HSN in 12 patients (48%), pathologic VIN in 7 (28%), and pathologic SVV in 5 (20%). Overall, 20 (80%) patients showed abnormal findings through a set of VFTs. Patients with an interaural difference of bone-conduction hearing thresholds ≥10 dB tended to show more abnormal VFT results than those for whom the interaural difference of bone-conduction hearing thresholds was <10 dB.
Conclusion
Our data show that one-fourth of patients with unilateral COM show abnormal caloric results on the COM side. However, subclinical latent vestibular imbalances were found to be common, which might be related to the gradual vestibular involvement in inflammatory processes, regardless of the caloric results. Results of a set of VFTs should be referred to when determining vestibular imbalance in patients with COM.
INTRODUCTION
Water caloric testing is generally considered to be contraindicated in patients with chronic otitis media (COM) and a closed-loop system or air caloric testing is an alternative. However, COM can alter the anatomy of the middle ear and even cause labyrinthine dysfunction, resulting in the question as to whether caloric results in patients with COM represent real vestibular function. There have been a few studies on the caloric test in patients with COM (1-4). It was reported that the size of the tympanic membrane perforation and a previous history of an ear operation can influence results of caloric testing (2). Thus, it is difficult to interpret caloric results in patients with COM, especially when they complain of dizziness or vertigo. Recently, it was reported that the incidence of abnormal caloric results among patients with COM was high and correlated well with abnormalities on rotational chair testing (3). It was reported that a set of vestibular tests can be helpful in detecting vestibular imbalances even in patients with vestibular neuritis who show normalized canal paresis in a follow-up caloric test (5). We wanted to investigate the results of various vestibular tests in patients with COM. The aims of the study were to evaluate the incidence of abnormal air caloric results and their characteristics in patients with unilateral chronic otitis media and without any history of vertigo, and to compare results of caloric testing with results of other vestibular function tests (VFTs).
MATERIALS AND METHODS
Twenty five consecutive patients with unilateral COM, who were scheduled for surgical intervention, were enrolled in this study. No patients had any ear surgery before, and there was no history of vertigo in their past medical histories. A history of intermittent dizziness was elicited from 4 (16%) of the 25 patients. However, it was not a primary complaint of any of the patients. All patients gave their consent to participate in the study, which was designed in accord with the guidelines of the local ethics committee. Patients were evaluated preoperatively via a medical history, and physical, audiologic and vestibular tests. Vestibular function was assessed using an air caloric test, a head-shaking nystagmus (HSN) test, a vibration-induced nystagmus (VIN) test, and a subjective visual vertical (SVV) test. Bone conduction hearing thresholds were obtained from both ears and the difference between the two ears was calculated. A positive difference between values meant that the COM-sided ear had a poorer bone conduction threshold than the intact ear.
The slow-phase velocity (SPV) of spontaneous nystagmus was determined as the average of the 3 fastest velocities, which were identified in a 10-sec time window while the subject was upright in the dark. A positive SPV value meant slow-phase eye movement to the COM-side, and vice versa.
An air caloric test was used. Eye movements were recorded by means of a video-based system (CHARTR VNG, ICS Medical, Schaumburg, IL, USA). Each ear was irrigated alternately with a constant flow of air at temperatures of 50℃ and 24℃, and for a constant period of time (60 sec). The maximum SPV of nystagmus was calculated following each irrigation, and Jongkees's formula was used to determine canal paresis (CP). It was considered abnormal if CP was ≥25%. A positive value meant CP on the COM-side.
The HSN test was performed with the patient sitting. The patient's head was vigorously rotated 20 times for 10 sec at 2 Hz, with a maximum amplitude of ~40° in the horizontal plane. After this, eye movements were recorded for 1 min. The maximum SPV after termination of head-shaking was calculated. A positive SPV value meant slow-phase eye movement to the COM-side. It was considered abnormal if the SPV was ≥4°/sec (6).
For the VIN test, we used a hand-held vibrator (VVIB 100, Synapsys, France) with a fixed frequency of 100 Hz. With the patient in the sitting position, eye movements during vibratory stimulation were recorded with a video-based system. Eye movement recordings were made and maximum SPV was calculated while vibration was applied to 4 different sites: right and left mastoid bones; right and left sternocleidomastoid muscles. The subject was instructed to continue to look straight ahead while the vibration continued for about 10 sec. The slow-phase velocity of VIN was determined as the fastest slow-phase velocity during vibration stimulation. A positive SPV value meant slow-phase eye movement to the COM-side. It was considered abnormal if all the SPVs from the four different stimulation sites were ≥2°/sec or SPVs from both mastoids or SCM muscles were ≥5°/sec, a value which we obtained from normal volunteers (7).
For the SVV test, the subjects were seated upright in a chair and their heads were stabilized using a neck rest. In front of the subjects was a computer monitor on which a dim white line was displayed in an otherwise darkened room. Subjects were asked to adjust the visual rod to the vertical position by manipulating a remote control held in both hands. When the line appeared earth vertical, the subject clicked an enter button, which would automatically calculate the deviation in degrees from the true gravitational vertical. The average of the 5 settings was used as the measure of SVV tilt. A positive value meant SVV tilt to the COM-side. It was considered abnormal, if the tilt was ≥2.7°, which exceeded the mean ±2 SD from 34 normal controls (8).
RESULTS
Spontaneous nystagmus of small amplitudes was observed in four patients. One (No. 14) showed SPV of 2°/sec towards the COM side and 3 patients (Nos. 5, 7, & 22) showed SPV of 1°/sec towards the intact side (Table 1). Canal paresis, SPVs of HSN, SPVs of VIN at 4 different stimulation sites, and the SVV tilts of each patient are shown in Table 1.
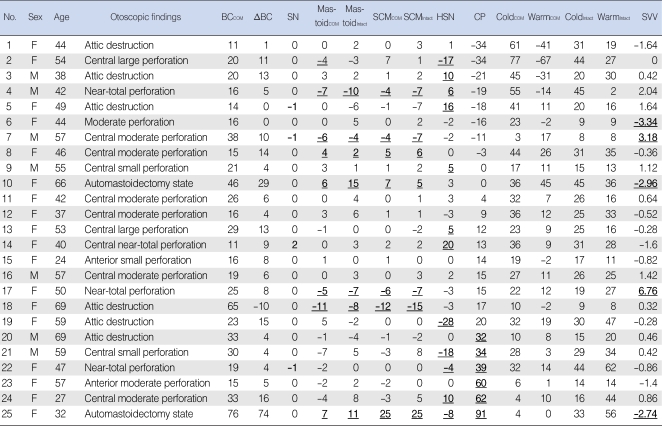
Tympanic membrane findings and results of audiological and vestibular tests in patients with unilateral chronic otitis media
Caloric canal paresis was pathologic (≥25%) on the COM side in 6 patients. There were two patients with pathologic CP on the intact side who showed inverted nystagmus upon warm air stimulation on the COM-sided ear (Fig. 1). The inverted nystagmus towards the intact side while the COM-sided ear was stimulated by warm air (observed in 4 patients, Nos. 1-4). Two patients also showed hyper-reactivity (SPV >60°/sec) to cold air stimulation on the COM-sided ear. Thus, we did not classify them as pathologic. They showed wide attic cholesteatoma or large perforation.

Paradoxical caloric responses. Inverted nystagmus was observed beating toward the non-stimulated side during warm air stimulation on the left ear (COM-sided) by evaporative cooling, followed by secondary nystagmus beating towards the stimulated side (patient No. 1). This inverted nystagmus and hyperactive responses to the cold air stimulation on the COM-side suggest that the COM-sided ear was hyper-excited. The dots indicate slow-phase eye velocities and a positive value means the direction of the slow-phase eye movement is to the right.
SPV: slow-phase eye velocity; COM: chronic otitis media.
Twelve (48%) showed abnormal HSN. Seven (58%) of 12 patients with pathologic HSN showed slow-phase eye movements towards the COM-side. However, the other 5 (42%) showed slow-phase eye movements towards the intact side. Seven (28%) showed abnormal VIN. Three (43%) of 7 patients with pathologic VIN showed slow-phase eye movements towards the COM-side and the other 4 patients (57%) showed slow-phase eye movements towards the intact side. Five (20%) showed abnormal SVV. Two (40%) of 5 patients with pathologic SVV showed SVV tilts towards the COM-side; the other 3 (60%) showed SVV tilts towards the intact side. Overall, 6 (24%) of 25 patients showed abnormal canal paresis, 12 (48%) showed abnormal HSN, 7 (28%) showed abnormal VIN, 5 (20%) showed abnormal SVV, and 20 (80%) of 25 patients showed an abnormal result in at least one vestibular function test. The pathologic sides according to various tests were not all the same in the patients. There was no difference in abnormal rates in other vestibular function tests between CP pathologic and normal groups (P>0.05, Fisher's exact test) (Table 2).

Relationship between the results of caloric and other vestibular function tests (n=25)
Bone-conduction hearing thresholds for the COM-sided ear were 11-25 dB nHL in 16 (64%), 26-40 dB nHL in 6 (24%), and more than 40 dB nHL in 3 (12%). Ten patients showed an interaural difference of BC thresholds ≥10 dB. They all showed an abnormal result in at least one vestibular test. Though the difference was not significant, patients with an interaural BC difference ≥10 dB tended to show more abnormal results in vestibular function tests than the others with an interaural BC difference <10 dB (P=0.06, Fisher's exact test) (Table 3). All four patients (Nos. 3, 14, 18, and 23) who complained of intermittent dizziness also had an abnormality in at least one vestibular test.
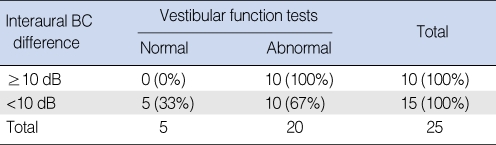
Relationship between the interaural difference of bone conduction (BC) hearing levels and the results of vestibular function tests (n=25)
DISCUSSION
We assessed vestibular function of patients using various vestibular tests, including air caloric, head-shaking nystagmus, vibration-induced nystagmus, and subjective visual tests. Caloric testing is the most widely used for identifying the presence of and the side of peripheral vestibular hypofunction. The caloric test probes lateral canal function mostly by causing convective endolymph movement (9). Vibration-induced nystagmus reflects a side difference of peripheral vestibular excitability, which means that an intact semicircular canal (SCC) is stimulated more than the lesioned side (7, 10-13). In patients with unilateral vestibular neuritis, the slow-phase eye movement of VIN was toward the lesioned side and the amplitude of SPV was correlated with canal paresis of the caloric test. It was assumed that the VIN test can probe lateral SCC function like the caloric test can (7, 14). Head-shaking nystagmus is induced by vigorous head shaking and generated by an asymmetric peripheral vestibular input and a central-velocity storage mechanism, which may perseverate the peripheral vestibular signals (15-17). It was reported that the perception of verticality (subjective visual vertical) largely depends on the otolith function (18). Normal subjects sitting upright in a dark room can correctly align a light bar with the perceived gravitational horizontal or vertical with an accuracy of ~3° but patients with unilateral vestibular lesions tilt the bar towards the side of the lesion (19).
In this study, air caloric tests had a side predilection for caloric paresis on the COM side. Our abnormal rate (24%) in caloric testing is less than that (76%) of an earlier report that pathologic the caloric response rate was high (3). Their high rate could be explained by their study population which was plagued with complex problems (13 bilateral COM, 3 semicircular fistulas, 2 stapes subluxation). Also, most of their patients had had previous ear surgeries and a history of dizziness/vertigo was elicited from 44% of them. Although anatomic changes can decrease canal responses to caloric stimulation on the COM-side in this study, it was reported that the COM-sided labyrinth can be influenced or gradually damaged by inflammatory processes (20-22). However, inverted nystagmus was an unexpected finding and may be an example of false information from the caloric test. The inverted nystagmus happened when the ear was stimulated by warm air caloric stimulation. It was reported that endolymph cooling due to evaporative cooling of the mucus or moisture lining the middle ear cavity by dry warm air stimulation is a possible mechanism for inverted nystagmus. This idea was supported by an experiment in which the inverted nystagmus disappeared when a warm air stimulus was saturated with water vapor (1). It was reported that patients with a large tympanic membrane perforation or an open mastoid cavity may show hyperactive caloric responses on the perforated side (2). In our study, the inverted nystagmus to the warm air stimulation was also accompanied by a hyperactive caloric response to cold air stimulation, leading to pathologic canal paresis on the intact side (patients Nos. 1-2). These findings confirm that direct exposure of the labyrinth to warm and cold air stimulation can induce this phenomenon. This means that the COM-sided ear was stimulated too much, resulting in canal paresis on the intact side and we should not consider these CP results pathologic. We could not find any patients who had real hypo-responsiveness on the intact-sided ear without these paradoxical responses.
Theoretically, the results of various tests can be different, depending on how many and which parts of peripheral vestibular organs are impaired. When we assume that any abnormal results indicate vestibular impairment, 20 of our patients (80%) can be interpreted as having vestibular impairment. A high rate of abnormal results in vestibular function tests in patients with COM was reported (3, 4). It can be argued that the sensitivity of the vestibular tests is too high; however, there is a report that pathological labyrinthine changes have been described in a high percentage of human beings affected by acute (82%) and chronic (77%) middle ear infections (20), although the incidence of clinical labyrinthitis is ~5% for otitis media (21, 22). It was also reported that vestibular imbalances can be detected in patients with unilateral vestibular hypofunction through a set of vestibular function tests, even when CP is normal, resulting in increased sensitivity for detecting a vestibular imbalance (5). Results of caloric test could be different from those of other tests in several ways. Vestibular tests probe different parts of peripheral vestibular organs, using various stimulating methods. Furthermore, these tests probe vestibular imbalance in different frequency ranges (5).
There is also a report that vertigo and dizziness are common in children with long-lasting middle ear effusion (23). Pathologic findings through electronystagmographic tests and the Bruininks-Oseretsky tests for motor proficiency were found in 58% of the children with chronic middle ear effusion, as compared with only 4% of the control group. The symptoms and signs of balance disturbances resolved in 96% of the children after ventilation tube insertion (23). In another study (24), children with otitis media had a higher velocity of sway than normal children indicating that episodes of otitis media may affect balance. In that sense, we suggest that the incidence of vestibular impairment in patients with unilateral COM is high, even though they did not complain of definite vestibular symptoms. Our findings that patients with an interaural BC difference ≥10 dB tended to show more abnormal results in vestibular function tests than those with an interaural BC difference <10 dB indirectly support the idea that a vestibular imbalance might be related to gradual vestibular involvement in inflammatory processes.
Although pathologic CP was always on the COM side except for patients with paradoxical responses, the sides of vestibular hypofunction according to other tests were not always on the COM side. These trends were seen during follow-up examinations in patients with vestibular neuritis at a compensated stage (5). In that study, even when canal paresis was normalized, other vestibular function tests could reveal the prior presence of a vestibular imbalance; however, no other vestibular tests than the caloric test can predict the side of vestibular hypofunction consistently (5). This can be explained by the fact that the caloric test is the only vestibular test which can probe unilateral vestibular function through unilateral caloric stimulation. The other tests used in this study probe vestibular imbalance through bilateral stimulation (VIN and HSN) or under a bilateral influence (SVV), which suggests that they are easily influenced by vestibular compensation. Peripheral recovery or central increase of VOR gain to the stimulation of the affected vestibular apparatus may explain this reversed direction (5, 17).
In summary, one-fourth of patients with chronic otitis media showed abnormal caloric results on the COM side; however, there were no cases with pathologic canal paresis on the intact side. Although paradoxical responses of the COM-sided ear can result in canal paresis on the intact side, this should not be interpreted as abnormal. Our data also show that latent subclinical vestibular impairment is relatively common in patients with chronic otitis media. This is possibly related to gradual vestibular involvement in inflammatory processes. Results of a set of VFTs should be referred to when determining vestibular imbalance in patients with COM.