The Allele 2 of the VNTR Polymorphism in the Gene That Encodes a Natural Inhibitor of IL-1β, IL-1RA Is Favorably Associated With Chronic Otitis Media
Article information
Abstract
Objectives
Chronic otitis media (COM) is followed by irreversible tissue damage and destruction of the middle ear structures, with the possibility of complications under the maintenance of inflammation. Inflammatory mediators such as cytokines play a crucial role in the initial stage of inflammation. The aim of this study was to evaluate the association of the polymorphisms in two innate immunity/inflammation cascade genes from interleukin-1 (IL-1) gene cluster with COM with regard to cholesteatoma.
Methods
In the cross-sectional case-control study, DNA samples were collected from 189 patients with COM and 119 controls from a population of Serbia. The +3953 C/T (rs1143634), TaqI polymorphism in interleukin-1 beta (IL-1β) gene and 86 bp variable number tandem repeat (VNTR, rs2234663) polymorphism in the IL-1 receptor antagonist (IL-1RA) gene were analyzed by polymerase chain reaction.
Results
The IL-1β TaqI polymorphism was not significantly different in patients compared with the control group. The significant difference between patients and controls was observed for both, genotype and allele frequencies of IL-1RA VNTR polymorphism (chi-square P<0.01). We found that carriers of IL-1RA allele 2 (odds ratio, 0.47; 95% confidence interval, 0.29 to 0.76; P=0.004) have a favorable association with COM, using multivariate logistic analysis that included both polymorphisms, age and sex. The IL-1RA allele frequency distribution was significantly different with regard to cholesteatoma.
Conclusion
The carriers of allele 2 of VNTR IL-1RA polymorphism had a decreased odds ratio for COM, which is in agreement with findings in other inflammatory disease and its previous association with higher IL-1RA levels. Possible down-regulation of IL-1 mediated proinflammatory signaling pathways via IL-1RA in COM as well as results of our study should be further investigated and replicated.
INTRODUCTION
Otitis media (OM) is a worldwide health problem with high prevalence, which consumes many medical resources. It is a multifactorial disorder in which bacterial infection plays an important role. Chronic otitis media (COM) is followed by irreversible tissue damage and destruction of the middle ear structures, with the possibility of complications under the maintenance of inflammation. To date, only few genetic studies have been performed in OM, but mostly in COM with effusion and recurrent OM (ROM), and the results have been ambiguous [1-5]. Inflammatory mediators such as cytokines play a crucial role in the initial stage of inflammation [1] caused by bacteria [6-8] and their role in OM have been suggested [9,10]. The interleukin-1 beta (IL-1β) is a mediator of both bacterial and viral OM and has influence on many different target cells, thus it stimulates proinflammatory network in the middle ear and could induce activation and proliferation of fibroblast and growth of osteoclasts in the middle ear possibly leading to fibrosis and bone erosion [1,11]. Cholesteatomas, the epidermal lesions in the middle ear that lead to erosion of bones, are commonly associated with ROM and often contains bacteria. It was recently shown that inflammation and innate immunity system play an important role in cholesteatomas, as well [12,13].
The number of studies revealed the association of IL-1 gene cluster with a predisposition to certain inflammatory diseases, but only a few had been performed in OM [14,15]. The genetic variant +3953 (rs1143634) in IL-1β has been suggested to influence production of IL-1β protein [16] while the variable number tandem repeat (VNTR) variant (rs2234663) in anti-inflammatory IL-1 receptor antagonist (IL-1RA, also called IL-1RN) has been proposed to influence expression of IL-1RA protein [17].
The aim of this study was to evaluate the association of the polymorphisms in two innate immunity/inflammation cascade genes from a single cluster (IL-1β +3953 C/T and IL-1RA 86 bp VNTR) with COM with regard to cholesteatoma. Bacterial flora and basic biochemical parameters were also analyzed with regard to the presence of cholesteatoma and genotypes of investigated polymorphisms.
MATERIALS AND METHODS
Subjects
This cross-sectional case-control study was approved by the Ethics Committee of the Clinical Center of Serbia (approval No. 29/VI-15). All participants (or parents of children) gave their signed informed consent for participation in the study.
All of the patients underwent surgery due to the symptoms of chronic middle ear disease. The 189 consecutive patients with COM without effusion were collected at the Clinic of Otorhinolaryngology and Maxillofacial Surgery, Clinical Centre of Serbia, Belgrade from 2011 to 2013 to participate in the study. The blood samples for genetic analysis were collected prior middle ear surgery. The children suspected of having head and neck anomalies, systemic disease or congenital or acquired immunodeficiency were excluded from the study. In order to evaluate the most common etiological agent in patients with multiple bacteria in cultures were excluded from the study. The patient group consisted of 34 children (aged between 2 and 18 years, mostly >5 years old) and 155 adults (aged 41±19 years). In children, male sex was predominantly present (61.76%) while in adults, females predominated (54.36%). In total, there were 47.08% males and 52.92% females in the patient group. According to the ear pathology group consisted of patients with nonsuppurative COM with tympanic membrane retraction without cholesteatoma, patients with suppurative COM and tympanic membrane perforation and patients with COM with cholesteatoma.
From the adults undergoing annual medical check-up at Occupational Medical Centers, Belgrade, Serbia, who underwent clinical and biochemical examination, 119 (aged 41±15 years) that were without previous history of COM and allergies and evidence of any chronic inflammatory disease such as, rheumatoid arthritis, systemic lupus or allergies, asthma, inflammatory bowel disease and Crohn disease, renal failure or diabetes mellitus were recruited as controls. In controls otomicroscopy, pure tone audiometry and tympanometry were done. The appearance of the tympanic membrane under a microscope was uneventful, audiogram showed normal hearing and type A tympanogram the proper mobility of the tympanic membrane. The results of these examinations have pointed to a healthy middle ear.
Diagnosis of COM was established by otomicroscopy, tympanometry in retracted tympanic membrane, pure tone audiometry in patients over five or objective audiometry in younger children. Computed tomography of temporal bone was performed in cholesteatoma patients. Patients with tympanic membrane retraction (COM non-suppurativa) underwent surgery using different techniques depending of retractions’ stage and auditory ossicle conditions. Retracted tympanic membranes were classified according to the Erasmus classification for pars tensa retraction and Tos classification for attic retractions [18,19]. The techniques used were aeration tube insertion alone for the first stage of retraction, or combined with resection of the retraction and grafting with cartilage or fascia, or only grafting. Patients with COM suppurativa underwent tympanoplasty wall up with antrotomy or mastoidectomy with tympanic perforation grafting [20]. Patients with cholesteatoma were treated with two stage tympanoplasty procedure. There were no positive data about allergy per anamnesis or clinical examination in the whole patient group. Samples of middle ear secretion were taken with sterile cotton swabs during surgery, and bacterial cultures were done immediately after sampling, inoculated to blood agar medium and MacConkey medium. The cultures were incubated for 24 hours at 35ºC, and bacteria were identified by Gram staining and biochemical tests. Standard biochemical measurements of blood parameters were performed for all patients.
Genetic analysis
Genomic DNA was isolated from peripheral blood samples collected with ethylenediaminetetraacetic acid and purified by the proteinase K/phenol extraction method. The +3953 C/T polymorphism in IL-1β gene and 86 bp VNTR polymorphism in the IL-1RA gene were analyzed by the polymerase chain reaction method on an ABI 9700 Thermal Cycler (GeneAmp; Applied Biosystems, Foster City, CA, USA) in a 20 μL reaction mixture containing 200 ng of genomic DNA using the following primers: IL-1β (forward 5´-GTATATGCTCAGTGTCCTC-3´ and reverse 5´-CATGGAGAATTAGCAAGCTG-3´), IL1-RA (forward 5´-CTCAGCAACACTCCTAT-3´ and reverse 5´-TCCTGGTCTGCAGGTAA-3´). The genotypes for IL-1β +3953 C/T, TaqI polymorphism were visualized on 8% polyacrylamide gel after overnight restriction digestion with TaqI enzyme and for IL-1RA 86 bp VNTR polymorphism on 1.8% agarose gel.
Statistical analysis
The frequencies of genotypes and alleles were determined by the gene counting method. To compare the obtained frequency distribution of genotypes in the control group with the expected values of the Hardy-Weinberg equilibrium, we applied the chi-square test. For test of independence between two categorical variables, the Pearson chi-square test was used. Multiple logistic regression analysis was performed in order to assess if IL-1β and IL-1RA polymorphisms are independently associated with susceptibility to COM (expressed in terms of adjusted odds ratio [OR] and its 95% confidence interval [CI]). In all tests, the value of P<0.05 was considered significant. All statistical analyses were performed using Statistica software 5.0 (Statsoft Inc., Palo Alto, CA, USA). The statistical power of the study for the observed effect of polymorphism on susceptibility to COM was calculated using the power and sample size calculation (v3.0.43) [21].
RESULTS
Genotypes and alleles in COM patients and controls
The prevalence of VNTR IL-1RA and IL-1β TaqI genotypes and alleles in COM patients and controls were shown in Table 1. We didn’t find the deviation from Hardy-Weinberg equilibrium in the investigated groups. Distribution of genotypes and alleles of IL-1β TaqI polymorphism were not significantly different in patients compared with the control group. The significant difference between patients and controls was observed for both, genotype and allele frequencies of IL-1RA VNTR polymorphism (P<0.01) (Table 1). By univariate analysis we calculated crude OR for IL-1RA allele 2 containing genotypes (OR, 0.48; 95% CI, 0.29 to 0.78; P=0.003), the IL-1 TaqI 22 genotype (OR, 1.36; 95% CI, 0.44 to 4.23; P=0.597), male sex (OR, 0.68; 95% CI, 0.41 to 1.10; P=0.114) and age (OR, 0.99; 95% CI, 0.98 to 1.01; P=0.473). We further found that IL-1RA allele 2 containing genotypes (OR, 0.47; 95% CI, 0.29 to 0.76; P=0.004) had an independent favorable association with COM, using multivariate logistic analysis that included polymorphisms (IL-1β TaqI and IL-1RA VNTR genotypes grouped with regard to allele 2 presence or absence), age and sex (Table 2). We had the study power of 86% for the observed association with an OR=0.47, at the significance level of 0.05 and the given sample size.

Genotype and allele frequencies of the IL-1RA VNTR and IL-1β TaqI gene polymorphisms in COM patients and controls

Odds ratio for COM in regard to IL-1RA VNTR genotypes grouped by allel 2 status
Genotypes and alleles in COM patients without cholesteatoma and COM patients with cholesteatoma
The prevalence of VNTR IL-1RA and IL-1β TaqI genotypes in COM patients without cholesteatoma and COM patients with cholesteatoma was not significantly different (Table 3). We found a significant difference in the IL-1RA VNTR allele frequency distribution between two groups of patients (P=0.034) (Table 3), with allele 1 predominance in COM patients without cholesteatoma and allele 2 predominance in COM patients with cholesteatoma. Subgroups of COM patients, those without cholesteatoma and those with cholesteatoma had significantly decreased IL-1RA allele 2 containing genotypes in comparison to controls (P=0.003 and P=0.021, respectively), but there was no difference between two groups of patients (allele 2+: non-cholesteatoma vs. cholesteatoma, 24.4% vs. 28.6%; P=0.560).
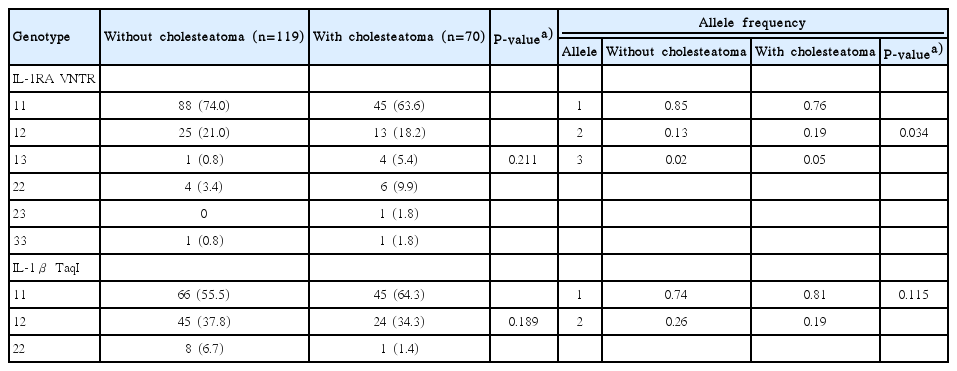
Genotype frequencies of the IL-1RA VNTR and IL-1β TaqI gene polymorphisms in COM patients with and without cholesteatoma
DISCUSSION
The aim of this study was to evaluate the association of the polymorphisms in two innate immunity/inflammation cascade genes from a single cluster (IL-1β +3953 C/T, TaqI and IL-1RA 86 bp VNTR) with COM with regard to cholesteatoma. Genes that control the production of cytokines are the first choice candidate genes for COM, same as for a variety of chronic inflammatory and autoimmune human diseases [22]. But up to date not many studies have been performed using a candidate gene approach for COM/ROM. The main finding of this study was that allele 2 of VNTR IL-1RA polymorphism was favorably associated with COM. Previously, only the Finnish study reported an association between IL-1α and ROM in children without allergic disorders [14]. The lack of association between IL-1β +3953 C/T polymorphism with COM, in this study, is in agreement with previous results [14,15]. Moreover, previously we didn’t find the association of this polymorphism with other chronic inflammatory disease, multiple sclerosis, in patients from Serbia [23]. Still, the association between acute OM symptom severity and IL-1β +3953 polymorphism, in a subset of children with more severe tympanic membrane involvement, was found recently [24]. In this study, we have shown the significant favorable effect of IL1-RA VNTR allele 2 toward susceptibility to COM, adjusted for IL-1β TaqI polymorphism, age and sex. Previously the same polymorphism has not been associated with recurrent acute OM in Finnish population [14]. The IL-1RA allele 2 was suggested to be associated with higher IL-1RA levels [17,25], which can lead to down-regulation of IL-1 mediated proinflammatory signaling pathways thus becoming the reasonable candidate gene in inflammatory diseases. It is known that complex formed by IL-1 cytokines and receptors recruits intracellular signaling, including MyD88-dependent activation of NF-κB, p38, JNK, and ERK [26]. Novel results showed that pathogens that causes pneumonia and OM, exert proinflammatory effects through the NF-κB pathway via TLR2, MyD88, and IRAK4 [27]. The IL-1RA after binding to IL-1 receptor does not activate intracellular signaling pathways thus exerts anti-inflammatory role. It was recently shown that blockage of the IL-1α/PI3K/NF-κB signaling pathway may be a major mechanism by which IL-1RA inhibits proinflammatory effects [28]. Recent meta-analysis in chronic periodontitis suggested a decreased risk for aggressive periodontitis in allele 2 carriers in Caucasians and significantly higher risk for chronic periodontitis in Asians [29]. It has been already known that IL1-RA VNTR allele frequency may vary by ethnicity and previously the association of allele 2 with chronic rhinosinusitis was found in Taiwanese, but not in Caucasians [30]. In multiple sclerosis, another chronic inflammatory disease, allele 2 had been associated with a more benign form of disease in patients from Italy [31] and had a protective role for its susceptibility in Serbian population [23]. Although IL-1RA has been present in the research of inflammatory disease for more than a decade only recently, it was thoroughly described as an active counterpart of IL-1β actions, which diminishes deleterious effects on metabolic processes in downstream organs and tissue damage [32]. Hereof we investigated its copy number variant with regard to cholesteatoma in patients with COM and we show the significant difference in allele frequency, with allele 2 predominance in COM patients with cholesteatoma. Molecular mechanisms and genetic basis of both, COM and cholesteatoma and their potential clinical aggressiveness are challenging subject in current research [33] and has yet to be resolved. Recently, an extensive review was published in order to gather existing literature regarding heritability of cholesteatoma [34]. The heritable component of cholesteatoma etiology was suggested, although insufficiency in relevant literature suggests the need for a stronger body of evidence.
The major limitation of most of the genetic studies in COM, including this study was the limited number of cases included. This should be overcome in future studies and multicentric approach would be the most valuable. The more genetic data we gather along with clinical data, the more about the genetic architecture of COM will be visible. COM is a complex and multifactorial disease with both genetic and environmental factors underlying its pathophysiology. The drawback inherent from analyzing the limited number of factors, as in this study and most of the studies up to date, should be overcome too, and the multifactorial models of COM susceptibility and complications should be defined. Nevertheless, the retrospectively calculated study power for the significant association (86%) suggests that current results should be taken into account for further research, primarily because the VNTRs, such as IL-1RA VNTR, were not investigated in the SNP genome wide association studies.
In conclusion, the carriers of allele 2 of VNTR IL-1RA polymorphism had a decreased risk for COM, which is in agreement with findings in other inflammatory disease and its previous association with higher IL-1RA levels. Possible down-regulation of IL-1 mediated proinflammatory signaling pathways via IL-1RA in COM as well as results of our study should be further investigated and replicated.
HIGHLIGHTS
▪ The allele 2 of interleukin-1 receptor antagonist variable number tandem repeat is favorably associated with chronic otitis media.
▪ The interleukin-1 receptor antagonist allele frequencies were significantly different with regard to cholesteatoma.
Notes
No potential conflict of interest relevant to this article was reported.
Acknowledgements
This research was conducted as part of the OI 175085, financed by the Ministry of Education, Science and Technological Development of the Republic of Serbia.