Clinical Manifestations of Recurrent Parotid Pleomorphic Adenoma
Article information
Abstract
Objectives
This study was undertaken to confirm the clinical characteristics of recurrent pleomorphic adenoma (RPA), and to identify those factors that affect the development of malignant transformation (MT) from RPA.
Methods
The medical records of 270 patients, who were operated upon for parotid PA, were retrospectively reviewed. The pathologic specimens of a selected series of 23 patients were reviewed for histologic subtype and microscopic multi-nodularity.
Results
Mean age of initial operation in RPA without MT (RPA-MT) group was significantly lower than that of primary PA group. Mean age of the revision operation in RPA with MT (RPA+MT) group was significantly greater than that of RPA-MT group. Mean interval from operation to recurrence shortened after each revision operation. The risk of MT and additional recurrence increased significantly with recurrence. In RPA-MT group tumor recurrence occurred in 21.4% of patients despite a clear resection margin.
Conclusion
The risk factors for MT may be an age of over 45 yr and multiple recurrences. However, younger patients are more at risk of recurrence. A clear resection margin cannot guarantee a cure in RPA, and it seems that parotid pleomorphic adenomas slowly gain malignant characteristics after repeated recurrences.
INTRODUCTION
Pleomorphic adenoma (PA) is the most common benign tumor of the salivary gland that comprises 70% of all salivary gland tumors. This very common tumor has a unique property that is not common to other benign tumors. Almost all PAs have focally thin capsules and 25% of all PAs demonstrate satellite nodules or pseudopodia (1). Since uncontrolled growth with invasion into adjacent tissue is a feature of the malignant tumor, the invasive characteristic of PA is quite interesting. Generally, the surgical technique is blamed for the recurrence of PA in the parotid gland. This may be partially true, but there are some reports suggesting that the invasive characteristic of the tumor cells also has a roll in recurrence (2-4).
The incidence of recurrence is 0-17% (5-7). Given that an appropriate operation has been performed, the recurrence rate is reported to be 2-5% (8). Compared with primary PA, a more judicious approach is required for recurrent pleomorphic adenoma (RPA) of the parotid gland for several reasons. RPA is difficult to operate on and the risk of facial nerve damage is higher. RPA often has multicentric lesions and is sometimes associated with malignant transformation (MT). The possibility of MT in RPA is reported to range from <10 to 40% (5). Considering that RPA is still a benign mass, multinodular change and higher chance of malignant transformation require a more complete explanation, other than just poor surgical technique.
Although many articles have addressed primary PA of the parotid gland, not many studies have focused on the RPA. The objective of the present study was to review the clinical manifestations of RPA and to identify those factors that affect the development of MT from RPA.
MATERIALS AND METHODS
Review of medical records
From January 1984 through December 2004, 270 patients diagnosed with PA or carcinoma ex PA of the parotid gland, and who had undergone an operation at the Department of Otorhinolaryngology, Seoul National University Hospital were included in this study. Medical records were retrospectively reviewed. The mean follow-up period was 108.1±79.5 months for the parotid PA patients. At initial operation, 252 patients were diagnosed as having parotid PA and 18 patients were diagnosed as having carcinoma ex PA. Of the 252 PA patients, 232 had no evidence of recurrence after the initial operation; these patients are referred to as the primary PA group. PA recurred in the remaining 20 patients (the RPA group). This group was further subdivided into two patient groups, i.e., those in whom PA remained benign (the RPA-MT group) and those who later developed MT (the RPA+MT group). The RPA-MT group was composed of 15 patients who underwent a total of 19 revision operations, and the RPA+MT group was composed of five patients who underwent a total of eight revision operations. Of the 20 patients in the RPA group, 14 were referred to us after an initial operation in another hospital, and six underwent a first operation at our institute.
Operations of the parotid gland were classified into five types: enucleation, excision, superficial parotidectomy, total parotidectomy and wide resection. Enucleation was defined as mass removal involving the dissection of the supracapsular plane with no resection margin, whereas excision was defined as leaving a few millimeters of resection margin to preserve the tumor capsule. Superficial parotidectomy was defined as complete superficial lobe removal and partial superficial lobe removal. Total parotidectomy was defined as total removal of the parotid gland and partial removal of the deep lobe with resection of the superficial lobe. Wide resection was defined as excision of the mass and limited neck dissection of level II neck nodes.
Review of pathologic specimens
Twelve pathologic specimens were available for histological review in the RPA-MT group. Eleven pathologic specimens were selected from age- and sex-matched patients in the primary PA group. No pathologic specimens were available for histological review in the RPA+MT group.
Histologic subtype was determined according to Seifert's classification (9). This classification is based on the proportions of stromal and cellular components. In type 1, 30-50% of the tumor mass is composed of stroma, and in type 2 this increases to >80%. On the other hand, type 3 is rich in cells (>80%) but poor in stroma, and type 4, like type 3, is also rich in cells and poor in stroma, but differs from type 3 because the epithelial component is uniformly differentiated. Indeed, type 4 resembles monomorphic adenoma.
The nodularities of these 23 specimens were also checked, and specimens were categorized as being of the single nodular type or the multi-nodular type based on its microscopic findings. A multi-nodular type was defined as a tumor with one or more satellite nodules beyond the mother nodule capsule, and the single nodular type was defined as a tumor without any satellite nodules.
Statistical analysis was performed using the Student's T, Mann-Whitney U, and Pearson's chi-square tests in SPSS ver. 12.0 (SPSS Inc., Chicago, IL, USA). P-values of <0.05 were considered significant.
RESULTS
Sex and age of patients
Sex ratios (male:female) were 76:156 in the primary PA group, 6:9 in the RPA-MT group and 3:2 in the RPA+MT group. The ratios were not significantly different. Mean age at initial operation was 40.0±13.8 in the primary PA group. Mean ages at revision operations were 30.4±9.3 in the RPA-MT group and 49.2±18.2 in the RPA+MT group. The mean age of the RPA-MT group was significantly lower than that of the primary PA group (P<0.01). In addition, mean age at initial operation in the RPA-MT group was 21.9±8.5 yr, which was also significantly less than that of patients in the primary PA group (P<0.01). The mean age in the RPA+MT group was significantly greater than in the RPA-MT group (P=0.02). A significant difference was found in the distribution of patients with MT when the RPA patient group was dichotomized about 45-yr age (P<0.01).
Types of operation
Details of the initial operations are listed in Table 1. Incidences of recurrence were 66.7% (8/12) for enucleation and excision, 1.9% (4/214) for superficial parotidectomy, and 21.7% (5/23) for total parotidectomy. Enucleation and excision were associated with a significantly higher possibility of recurrence compared to superficial parotidectomy (P<0.01), given that the tumor sizes and locations were similar.

Types of initial operation
Details of subsequent operations due to recurrence are listed in Table 2. Because the majority of patients in the RPA+MT group had already undergone total parotidectomy during the initial operation, recurrence was mainly managed by excision or wide resection.
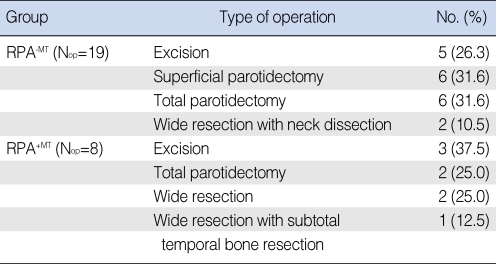
Operations performed to manage recurrent pleomorphic adenoma
Resection margins and surgical outcomes
Unfortunately, we were unable to check resection margins at initial operations in the RPA group, because the majority of the patients concerned had undergone an initial operation at another institute prior to their referral. As for the revision operations, in the RPA-MT group a clear resection margin was obtained in 14 (73.7%) revision operations, resection margins showed tumor involvement in four (21.1%) revision operations, and information was not available for one. Of these 14 revision operations with a clear resection margin, three (21.4%) later re-recurred. Of the four patients with a positive resection margin, two (50.0%) underwent adjuvant radiation therapy and have remained disease free for 9 and 92 months, respectively. One patient developed recurrence but follow-up was not possible, and the other patient who underwent an additional resection remained disease free at 84 months postoperatively. In the RPA+MT group a clear resection margin was obtained in five of the eight revision operations (62.5%). However, only one (20%) of the five did not recur (over a 9 month follow-up), and the four (80%) remaining patients expired due to the disease, despite a clear resection margin. All of the patients with a positive resection margin expired due to the disease.
Time to recurrence
Times between operation and recurrence were evaluated. The average times from operation to succeeding recurrence after operations 1-4 were 51.4, 27.5, 19.0, and 5.8 months, respectively (Fig. 1), which represented decreasing tendency after subsequent revisions. But the statistical significance was marginal (P=0.06).
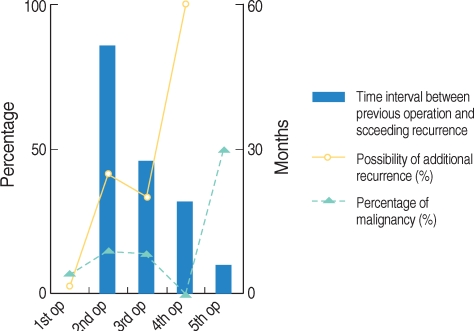
Progressive changes in clinical manifestations after multiple recurrences.
Duration between revision operations and subsequent recurrences tended to shorten as the number of previous revisions increased (P=0.06). The percentage of patients with a malignant tumor at revision surgery was higher than at initial operation (P=0.04). The general trend toward an increased risk of further recurrence after repeated surgery was significant (P<0.01), despite our finding of a lower risk at the third than at the second operation.
Percentage malignancy
Percentage malignancies among previously benign PA patients at operations 1-5 were 6.7% (18/270), 15.0% (3/20), 14.3% (1/7), 0.0% (0/2), and 50.0% (1/2), respectively (Fig. 1), which represented a significant increasing trend (P=0.04).
Possibility of additional recurrence
Additional recurrences in patients with benign PA after the operations 1-4 were 2.5% (6/252), 41.2% (7/17), 33.3% (2/6) and 100.0% (2/2), respectively (Fig. 1). A general trend was observed toward a higher possibility of recurrence after repeated operations (P<0.01).
Histologic subtype and nodularity
PA histologic subtypes were reviewed in the primary PA group and in the RPA-MT group. Results are presented in Table 3. No significant subtype distribution differences were observed between these two groups (P=0.57). As for nodularity, whereas only 45.5% (5/11) specimens were multi-nodular in the primary PA group, 91.7% (11/12) specimens were multi-nodular in the RPA group (P=0.03).
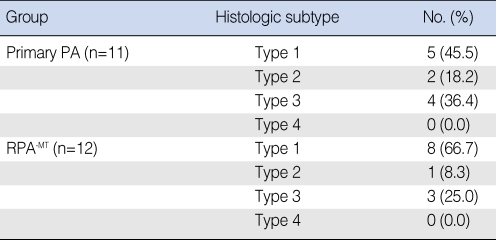
Histologic subtypes of pleomorphic adenomas
DISCUSSION
Although the knowledge of "pseudopods" and the introduction of "superficial parotidectomy" have greatly reduced the incidence of recurrence from 40% to <5% (10, 11) several questions remain unanswered about the manifestations of RPA, such as those concerning multi-nodular change and nodular infiltration into normal parotid tissue after recurrence (8). Until now, the rupture or spillage of tumor cells has seemed like a good explanation, but recent reports have suggested that there is no relationship between rupture and recurrence (12-14). Intriguingly, several studies have also reported that recurrence is more frequent in those treated by formal parotidectomy rather than in those that have undergone simple excision (15, 16). Distant metastasis of this benign tumor has also been reported on several occasions (17, 18). A new concept is needed to overcome these discordances. One suggestion made was that the biology of tumor cells might in part determine the development of recurrence and the multi-nodular appearances of masses. That is, PA tumor cells might adopt a more aggressive phenotype after recurrence (3, 19).
Age is related with recurrence and MT
On comparing the mean ages of the study groups, it was noticeable that patients in the RPA-MT group were significantly younger than in the primary PA group. There are several possible explanations for this observation, i.e., PAs in younger patients may be more aggressive than that in older patients (20), alternatively, as younger patients have a longer life span they are at greater risk of recurrence. However, in the present study, both age at revision operation (30.4±9.3 yr) and age at initial operation (21.9±8.5 yr) in the RPA-MT group were significantly lower than that in the primary PA group (40.0±13.8 yr). Therefore, it may not be true that a band of patients in the primary PA group, who have under gone an incomplete operation, will later turn into a member of the RPA-MT group. The characteristics of tumors in these two groups may be intrinsically different.
It was also noticeable that older patients had a higher probability of developing MT, as a significant difference was found in the distribution of patients with MT when the RPA patient group was dichotomized about 45 yr of age.
A clear resection margin may not guarantee a cure
Although RPA is generally considered a benign tumor, in the present study a clear resection margin was not found to guarantee cure, because in our RPA-MT group tumor recurrence occurred in 21.4% of patients despite a clear resection margin. Moreover, in the RPA+MT group, resection margins were found to be even less reliable, because tumors recurred in 80.0% of patients with margins found to be clear. Thus, even though RPA is considered a benign disease, surgeons should not rely wholly on pathologic conclusions concerning resection margins, and patients should be followed regularly after revision surgery.
Tumors may became progressively more aggressive after multiple recurrences
As Fig. 1 shows, time from operation until the next recurrence was reduced after repeated recurrences. The mean time to first recurrence was 51.4 months and that to second recurrence was 27.5 months. These results concur with those of Fee et al. (21), who found mean times to first recurrence of 5-7 yr and to second recurrence of 2-5 yr. In addition, in the present study, the likelihood of MT after repeated recurrence and likelihood of a subsequent recurrence also increased significantly with operation number. These results reveal that tumors become more aggressive after repeated recurrence.
RPA are more multi-nodular than is evident by intraoperative gross inspection
In terms of nodularity, 91.7% of RPAs were found to be multinodular under the light microscope, but previous intraoperative visual inspection findings place the figure at 44-67% (22, 23). Our findings indicate that although RPAs may appear to be single masses by gross inspection, the majority are microscopically multi-nodular with satellite nodules. Importantly, this finding provides good evidence supporting a wide resection approach, even for RPAs with an innocuous appearance.
In terms of Seifert's histologic subtypes, several reports have concluded that recurrence is higher for the type 2 subtype (9, 24, 25). According to these reports, 61% of RPA cases were of the type 2 subtype (25). However, in the present study, we were unable to find a significant difference between the primary PA and RPA groups with respect to subtype proportions, and the study by Fee et al. (21) also concurs with our findings. Thus, because of the above discrepancies it is difficult to give an overview of the relationship between recurrence and histologic subtype for now.
The results of this study indicate that RPA lies somewhere between a benign and malignant disease. Poor surgical technique has been generally blamed for recurrence, but the inherent nature of this tumor probably plays an important role even in the initial operation as well as the revision operation. For example, a more meticulous resection is required in younger patients since the nature of PAs in younger patients may be more aggressive than that in older patients. Based on our findings, the risk factors for MT seems to be an age of more than 45 yr and multiple recurrences. Also, it should be born in mind that tumors may become progressively more aggressive after multiple recurrences, and that RPA are much more multi-nodular to a great extent than is evident by intraoperative gross inspection.