Transcanal Endoscopic Tympanoplasty for Pediatric Patients Under 15 Years of Age With Chronic Otitis Media
Article information

Abstract
Objectives.
To evaluate the results of transcanal endoscopic tympanoplasty for pediatric patients with chronic otitis media (COM) and compare them to that of the previously standard microscopic assisted tympanoplasty technique.
Methods.
The patients were divided into two groups based on the operative method. Group 1 underwent tympanoplasty with a totally endoscopic assisted technique (n=21, 24 ears), and group 2 underwent tympanoplasty with the conventional microscopic technique (n=14, 15 ears). We used a transcanal approach in group 1 and a postauricular approach in group 2. In group 1, there were 15 cases of simple COM and nine cases of adhesive otitis media. In group 2, only 15 cases of simple COM were present. We analyzed the outcomes in terms of the hearing gain according to the surgical method and COM type, operation time, hospital stay after surgery, and graft success rate.
Results.
Postoperative hearing gain results including air conduction (AC) thresholds and air-bone gap (ABG) were not significantly different between the two groups (P>0.05). In both the groups, significant improvement in the postoperative AC and ABG was observed compared to the preoperative hearing. The hospital stay after surgery was significantly shorter in group 1 than the group 2: 2.1±0.4 days and 4.8±0.9 days (P<0.001), respectively. The intact graft success rate was 91.6% in group 1 and 93% in group 2; the values were not significantly different (P>0.05). There was neither intra- nor postoperative complications.
Conclusion.
Transcanal endoscopic ear surgery technique is more conservative than microscopic approach and can be performed in pediatric patients under 15 years of age with COM. Moreover, it offers similar surgical results compared to traditional microscopic technique, and a shorter operative time and hospital stay after surgery are the advantages of this technique.
INTRODUCTION
Surgical treatment of chronic otitis media (COM) has gloriously developed after the incorporation of the surgical microscopy in the 1950s [1]. Most of the otolaryngologists still prefer surgery with the microscope. Middle ear surgery using endoscopy was initiated in the 1960s. Initially, surgeons who were more used to microscopic manipulation felt uncomfortable in avoiding the use of endoscopy. However, numerous reports have been published on the use of endoscopy and the interest and importance of the endoscopic middle ear surgery have been revealed [2-5].
In cases with pediatric COM, many surgeons prefer a postauricular approach due to the narrow external auditory canal (EAC). However, transcanal approach using endoscope provides many advantages including, visualizing more details with wider view, less invasive eradication of the disease, middle ear reconstruction, and capable operation with narrow EAC. It is hypothesized that in some way or either endoscopic surgery might substitute former microscopic operation [6,7]. Herein, we have investigated the results of endoscopic transcanal tympanoplasty in pediatric patients aged below 15 years and attempted to explore the benefits of the technique.
MATERIALS AND METHODS
Operative instruments
For pediatric surgery, usually, more slender and shorter endoscope is used compared to sinus endoscopic surgery. We mostly used endoscope measuring 0°, 2.7 mm in diameter and 11–14 cm in length. The endoscope measuring 30°, 3.0 mm in diameter, and 14 cm in length was used additionally if needed. Similar surgical instruments were used for the previous microscopic middle ear surgery.
Subjects
Pediatric patients under the age of 15 years who underwent type I tympanoplasty from November 2008 through August 2017 were enrolled in the study. All the operations were done by one surgeon (HHC). Patients were divided into two groups depending on the operative method. There were 21 subjects (24 ears, group 1) with the endoscopic transcanal approach and the remaining 14 subjects (15 ears, group 2) were with microscopic postauricular approach.
Mean age of group 1 patients was 10 years (4–15 years). Simple COM was 15 ears and adhesive otitis media were nine ears. The mean age of group 2 patients was 11 years (6–15 years) and all were simple COM. There were no significant differences in the size of the perforation between the two groups (Table 1). The study was approved by the Institutional Review Board of Chonnam National University Hospital (IRB No. CNUH-2019-060).
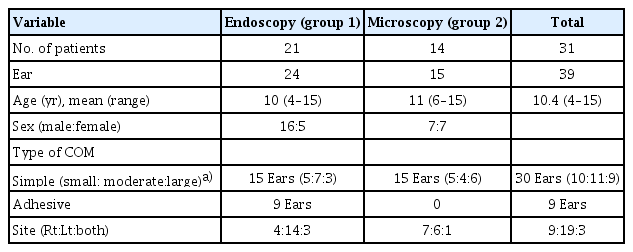
Demographic characteristics of patients
Operation procedure
For endoscopic surgery (group 1), general anesthesia was administered to 20 cases and local anesthesia to four cases. In all the cases, transcanal approach with 2% lidocaine and 1:100,000 epinephrine mixed solution injection on 3, 6, 9, and 12 o’clock position of the EAC was performed. Temporalis fascia harvest was done at 1 cm above the superior margin of the auricle. Cartilage and perichondrium were collected from the tragus. The endoscope was held by the left hand and surgical instruments were inserted by sliding by the EAC with the right hand. First, perforated tympanic membrane margin was trimmed with a sharp pick. EAC canal incision was done starting from 6 o’clock to the 12 o’clock position. EAC canalomeatal flap was elevated to gain entry into the tympanum. Pathologic lesion in the tympanum was checked and removed. Perforation was reconstructed with the harvested fascia and supported by gel foam (Fig. 1). In the case of tympanoplasty using the cartilage, the adhered tympanic membrane was separated from the promontory and then cartilage and perichondrium were placed underneath. In all the cases of microscopic surgeries (group 2), general anesthesia with conventional tympanoplasty with postauricular approach was administered except for two cases of near total perforation. In this cases, cartilage tympanoplasty was performed. (Table 2).

Transcanal endoscopic tympanoplasty. (A) Preoperative tympanic membrane shows moderate perforation and marginal thickening. (B) Endoscopic view of the eardrum during surgery after performing marginal trimming. (C) Entering the tympanum after the elevation of a tympanomeatal flap. (D) Grafting of temporalis fascia.

Operation methods and success rate
Comparison of the postoperative results
In order to investigate the utility of endoscopic transcanal tympanoplasty in pediatric patients, conventional microscopic surgery was set up as the control group. Postoperative hearing gain, postoperative hospitalization duration, and success of the tympanic membrane reconstruction were compared between the two groups. For statistical analysis, paired and independent t-test was performed by IBM SPSS ver. 19.0 (IBM Corp., Armonk, NY, USA). A P<0.05 was defined as statistically significant value.
RESULTS
Postoperative hearing improvement
Improvements in postoperative air conduction (AC) and air-bone gap (ABG) were compared between the two groups and no statistical significance was observed (P>0.05). Both groups showed significant hearing gain after surgery (P<0.05). AC gain in group 1 was 6.70±2.82 dB (P=0.045) and group 2 was 10.64±4.70 dB (P<0.001). Improvement in ABG was 5.74±7.97 dB in group 1 (P=0.009) and 8.97±3.51 dB in group 2 (P<0.001). Hearing gain according to the type of COM was also compared. Simple COM with endoscopic surgery showed 12.19±10.58 dB gain in AC (P=0.009) and 8.54±8.80 dB gain in ABG (P=0.018). In the case of adhesive otitis media with tympanoplasty using cartilage graft in all the cases, AC revealed 2.30±12.76 dB (P>0.05) gain and ABG revealed 3.50±6.42 dB gain (P>0.05). There were no statistically significant differences in hearing improvement in patients with simple COM between the two groups (P>0.05) (Fig. 2).
Hearing results according to operation method and type of chronic otitis media (COM). (A) Air conduction (AC) hearing results. (B) Airbone gap (ABG) hearing results. All data are average values of each group.
Operation time
Operation length was calculated when the patient was present in the operation room. In group 1 with endoscopy, general anesthesia was administered to 17 patients (20 ears) and local anesthesia to four patients (four ears). In group 2 with microscopy, general anesthesia was administered to 14 patients (15 ears). In case of patients who underwent surgery for both the ears, total time was divided into half for each ear for the purpose of calculation. Mean operation time was 73.3±17.8 minutes in group 1 and 90.3±13.8 minutes in group 2. The endoscopic group showed statistically meaningful less operative duration (P=0.002). Even for only general anesthesia cases, group 1 spent 77.0±17.1 minutes in the operation room, which was less when compared to group 2 (P=0.018) (Fig. 3).

Average operation time. Operation time is defined as the time that the patient has been in the operation room using nursing record.
Hospitalization duration and Neodrum success rate
The endoscopic group was hospitalized for mean 2.1 days (1–3 days) and microscopic group for 4.8 days (3–6 days). Hospitalization duration was shorter in the endoscopic group (P<0.001) (Fig. 4). Typically, 22 ears in group 1 (91.6%) and 14 ears in group 2 (93%) did not show any reperforation more than 1 year after the surgery.

Average postoperative admission days.
DISCUSSION
The goal for the COM treatment is the elimination of otorrhea and improvement in hearing ability. These are especially important in the pediatric population due to that COM can result in life-long hearing loss [8,9]. In pediatric patients, retroauricular approach using microscopy is commonly incorporated as they have narrower EAC compared to the adults. The retroauricular incision is associated with increased postoperative pain and hospitalization. Thus, it is always a problem for pediatric cases.
Moreover, microscopic surgeries that are usually used until now creates difficulties in exposing specific region like the anterior portion of the tympanum in cases with bulging anterior EAC. On the other hand, the endoscope can slide directly into the narrow EAC and provide a wider overall view of the tympanum. Disease eradication and tympanic membrane reconstruction after more detailed inspection are possible compared to conventional microscopic approach [6,7,10].
The advantage of the endoscopy for middle ear surgery is minimal invasiveness. Also, less damage to the normal tissue can be achieved with less operation time [11]. In the current study, no statistical difference in hearing improvement between endoscopic and microscopic groups was observed. In the case of adhesive otitis media, hearing gain was not as high as compared to the microscopic group, which could be due to the adhesive pattern of the disease instead of the operative mean. With respect to operation time, the endoscopic group showed a shortened duration as postauricular incision and reclosure were avoided. Postoperative hospitalization time was reduced in the endoscopic group owing to the absence of postauricular incision and minimizing normal tissue damage. Postauricular incision, which is commonly used in childhood COM surgery using microscope, causes postoperative pain and needs dressing of the surgical site, leading to longer hospital stay. This result coincides with the outcomes of other reports on pediatric endoscopic COM surgery [12-14].
Endoscopic tympanoplasty in the pediatric group provides a wider view compared to the conventional microscopy and creates possibilities in pediatric patients with narrow EAC. The technique demands for less soft tissue resection resulting in less operation time, less invasiveness, and less hospitalization duration. Endoscopic tympanoplasty is proposed as a good alternative to the microscopic approach in pediatric patients.
HIGHLIGHTS
• When tympanoplasty is performed in pediatric patients, endoscopy provides a wider view compared to the conventional microscopy and enables the transcanal approach in pediatric patients with narrow external auditory canal.
• Improvements in postoperative air conduction and air-bone gap were compared between the endoscopic group and microscopic group, and no statistical significance was observed (P>0.05).
• Compared the operation time between two groups, the endoscopic group showed statistically meaningful less operative duration (P=0.002).
• Hospitalization duration was shorted in the endoscopic group (P<0.001).
Notes
No potential conflict of interest relevant to this article was reported.
AUTHOR CONTRIBUTIONS
Conceptualization, Methodology, & Project administration: HHC. Data curation, Formal analysis, & Visualization: SL. Writing - original draft, review & editing: all authors.
Acknowledgements
This study was supported by a grant from Chonnam National University Hospital Biomedical Research Institute (No. BCRI 18009), Gwangju, Korea.