Statistical Analysis of Pure Tone Audiometry and Caloric Test in Herpes Zoster Oticus
Article information
Abstract
Objectives
Pure tone audiometry and caloric test in patients with herpes zoster oticus were performed to determine the biologic features of the varicella zoster virus (VZV) and the pathogenesis of vestibulocochlear nerve disease in herpes zoster oticus.
Study Design
A retrospective chart review of 160 patients with herpes zoster oticus was designed in order to determine the classic characteristics of vestibulocochlear nerve disease associated with the syndrome. Speech frequency and isolated high frequency acoustic thresholds were analyzed based on severity of facial paralysis and patient age. Patients without cochlear symptoms were selected randomly, and audiological function was evaluated. Patients with symptoms of vestibular dysfunction underwent the caloric test, and canal paresis was analyzed according to the severity of facial paralysis and the age of each patient.
Results
Among the 160 patients, 111 exhibited pure tone audiometry; 26 (79%) of the patients with cochlear symptoms and 44 (56%) of the patients without cochlear symptoms had abnormal audiological data. Among the patients without cochlear symptoms, 15 (19%) had hearing loss at speech frequency, and 42 (54%) had hearing loss isolated to high frequency. The incidence of cochlear symptoms in herpes zoster oticus was not related to the severity of facial paralysis. The incidence of patients with isolated high frequency hearing loss statistically increased with age, however the incidence of patients with speech frequency hearing loss did not increase. Thirteen patients complained vertigo, and the incidence of vestibular disturbances and the value of canal paresis in the caloric test increased to statistical significance in parallel with increasing severity of facial paralysis.
Conclusion
Mild or moderate cochlear symptoms with high frequency hearing loss were related to age, and severe vestibular symptoms were related to the severity of facial paralysis after onset of herpetic symptoms. This study might suggest us a clue to the pathogenesis of vestibulocochlear nerve disease in herpes zoster oticus.
INTRODUCTION
In 1907, James Ramsay Hunt first postulated that the etiology of herpes zoster oticus was the reactivation of the varicella zoster virus (VZV) in the geniculate ganglion (1). He described a variety of clinical manifestations of the syndrome that were ultimately named after him (2).
Although Ramsay Hunt Syndrome is now defined as herpes zoster oticus and facial paralysis, Hunt originally noted other symptoms and signs, such as tinnitus, hearing loss, nausea, vomiting, vertigo, and nystagmus. He explained that these additional symptoms were the result of the close proximity of the geniculate ganglion to the eighth cranial nerve within the bony facial canal (3).
In patients with herpes zoster oticus, disorders of the eighth cranial nerve are frequently observed. Hearing loss is usually mild to moderate, and the audiological data suggest cochlear and/or retrocochlear involvement (4). The vestibular symptoms are sometimes severe, and a recent study showed that both the superior and inferior divisions of the vestibular nerve could be widely affected (5). Evidence of inflammation within the auditory and vestibular nerves and the labyrinth has been noted on postmortem examinations of patients with herpes zoster oticus (6).
Recently, Kuhweide et al. (7) reported that the infection may spread to the cochleovestibular system through the vestibulofacial communicating branch or via perineural tissues within the internal auditory canal. Murakami et al. (8) also reported that the presence of VZV in the middle ear mucosa of patients with herpes zoster oticus suggested the arrival of VZV in the labyrinth through dehiscence of the facial nerve canal, creating a passage through the oval and/or round window. However, there are no studies to our knowledge that have stressed audio-vestibular findings related to the biological features of latent reactivated VZV and the anatomical structures around the eighth nerve.
This study focused on the audio-vestibular findings by pure tone audiometry and caloric test of patients with herpes zoster oticus. The findings were compared with the clinical severity of facial paralysis and patient age to clarify the pathogenesis of vestibulocochlear nerve disease in herpes zoster oticus.
MATERIALS AND METHODS
The charts of 169 patients with herpes zoster oticus in Yonsei University Health System between March, 1990 and March, 2007 were reviewed. The patients who had prior histories of hearing impairment or vertigo due to other causes were excluded from this study. The patients were classified according to severity of facial paralysis, based on the system proposed by House and Brackmann.
Patients with symptoms of cochlear dysfunction (hearing impairment, tinnitus, and ear fullness) underwent audiological tests. Pure tone audiometry was conducted at frequencies of 0.25, 0.5, 1, 2, 4, and 8 kHz. Acoustic thresholds of the affected ears were compared with those of the contralateral (unaffected) ears at each frequency level. The mean acoustic thresholds in speech frequency (0.5 kHz+1 kHz+2 kHz/3) and isolated high frequency (4 kHz+8 kHz/2) were calculated according to the severity of facial paralysis and patient age. Patients without cochlear symptoms were selected through a randomized pattern, and audiological function was evaluated as in the patients with cochlear symptom.
For the exclusion of age-related sensorineural hearing loss in older patients, the audiometric data of the affected ear were compared to those of the unaffected ear, and the patients who had hearing loss in the affected ear greater than 10 dB as compared to the unaffected ear were only included in this study.
Patients with symptoms of vestibular dysfunction underwent the caloric test as soon as possible after vestibular symptoms appeared. The patients who had vertigo with canal paresis more than 25% in the affected ear on caloric test were included in this study. Canal paresis was analyzed according to the severity of facial paralysis and patient age. The days following onset of vestibular symptoms, before or after onset of facial paralysis, were recorded.
RESULTS
Statistical analysis of pure tone audiometry in patients with herpes zoster oticus
Among the 160 patients whose records were obtained, 111 had audiometry findings consistent with herpes zoster oticus. Sixty-five patients were male (59%) and 46 were female (41%), with a mean age of 44.7±15.5 years. Thirty-three of those patients had complained of cochlear symptoms: hearing loss, ear fullness, tinnitus, or hyperacusis; all patients had sensorineural hearing loss with no conductive element. The number of randomly selected patients without cochlear symptoms who underwent audiological evaluation was 78.
The mean acoustic thresholds and standard errors at 0.25, 0.5, 1, 2, 4, and 8 kHz in the affected ear were calculated to be compared with those of the unaffected ear (Fig. 1). The mean acoustic threshold at all frequencies examined exhibited a statistically significant difference between the affected ear and the unaffected ear. The difference in the mean acoustic threshold between the two increased in parallel with frequency, to statistical significance (P<0.001, analyzed by repeated ANOVA test). More severe hearing loss was evident at high frequencies (4 kHz and 8 kHz) in the affected ear.
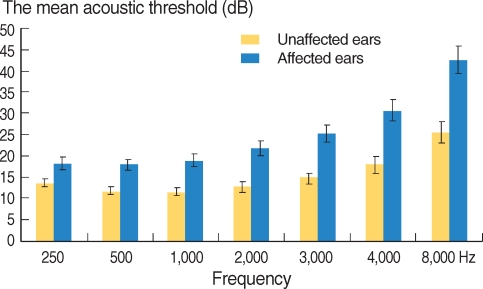
The mean acoustic threshold and standard errors of affected ears and unaffected ears of 111 patients with herpes zoster oticus. The mean acoustic threshold at all frequencies showed a statistical difference between the affected ear and the normal ear. The difference of mean acoustic threshold between the affected ear and the unaffected ear increased as examination frequency was made higher.
Among 33 patients with cochlear symptoms, 22 patients were male (67%), and 11 were female (33%), with a mean age of 47±15.5 years, ranging from 23 to 76. Among 78 patients without cochlear symptoms, 65 patients were male (59%), and 45 were female (41%), with a mean age of 42±15.5 years, ranging from 16 to 77.
The mean age of patients with cochlear symptoms was older than that of patients without cochlear symptoms (P=0.04), with no statistically significant differences noted between the two groups with regard to gender and severity of facial paralysis. There was a statistically significant difference between the two groups with regard to the mean acoustic threshold at all frequencies in the affected ear.
The values for mean hearing loss and standard errors at 0.25, 0.5, 1, 2, 4, and 8 kHz for the two groups are shown in Fig. 2. The audiological pattern in patients with cochlear symptoms was found to be present at all frequencies (mean hearing loss value higher than 10 dB) with statistically significant difference when compared to patients without cochlear symptoms. However, the mean hearing loss in patients without cochlear symptom at 4 kHz and 8 kHz was found to be higher than 10 dB.

The comparison of the mean hearing loss level in affected ear at 0.25, 0.5, 1, 2, 4, and 8 kHz between patients with cochlear symptoms and patients without cochlear symptoms. Statistically significant difference was demonstrated between the two groups at all frequencies examined. However, the mean hearing loss values in patients without cochlear symptoms at 4 kHz and 8 kHz was found to be higher than 10 dB.
The total number of patients with cochlear symptoms who had mean hearing loss more than 10 dB at speech frequency or isolated high frequency was 26 (79%). However, 44 (56%) of 78 patients who had not complained of cochlear symptoms exhibited mean hearing loss of more than 10 dB at speech frequency or isolated high frequency (Table 1). There was a statistically significant difference in the incidence of patients with mean hearing loss more than 10 dB at speech frequency between the two groups, but no difference at isolated high frequency. Among the patients without cochlear symptoms, 15 (19%) had hearing loss at speech frequency, and 42 (54%) had hearing loss at isolated high frequency. There was no patient who exhibited hearing loss at speech frequency without hearing loss at high frequency in either group.

Statistical comparison of incidence between the patients with cochlear symptoms and without cochlear symptoms in herpes zoster oticus
The mean age and standard deviation of patients included in this study was 42.9±15.6 years. With age, the incidence of herpes zoster oticus and cochlear symptoms in herpes zoster oticus patients did not increase (P=0.34). However, with age, the incidence of patients with isolated high frequency hearing loss increased, while the incidence of patients with speech frequency hearing loss did not (Table 2).
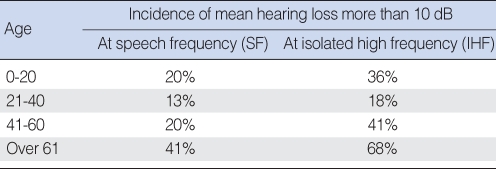
The comparison of incidence of patients with mean hearing loss more than 10 dB at speech frequency and at isolated high frequency according to age
The incidence of cochlear symptoms in patients with herpes zoster oticus was not related to the severity of facial paralysis (no statistical significance). The audiological data in patients with herpes zoster oticus were shown to be independent of the severity of facial paralysis (Table 3).

The comparison of incidence of patients with mean hearing loss more than 10 dB at speech frequency and at isolated high frequency according to the severity of facial paralysis
The caloric test in patients with herpes zoster oticus who complained of vertigo
Among the patients who had complained of vertigo or dysequilibrium, 13 had abnormal canal paresis (more than 25%) on caloric test. In all of them, facial paralysis and vesicular eruption were followed by severe vestibular disturbance. The incidence of vestibular disturbance and the severity of canal paresis in the caloric test increased in a statistically significant manner with increasing severity of facial paralysis (Table 4). The incidence of vestibular symptoms was lower than that of cochlear symptoms, and most vestibular symptoms occurred in cases of severe facial paralysis.
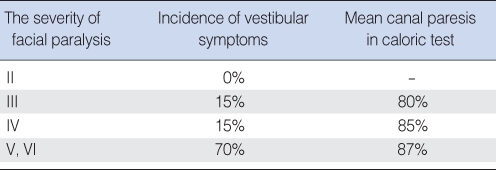
The incidence of vestibular symptoms and mean canal paresis according to the severity of facial paralysis
DISCUSSION
Many reports concerning vestibulocochlear nerve disease associated with herpes zoster oticus state that the classic syndrome described by Ramsay Hunt is not common and is no doubt a more complicated disease than the original description as "geniculate ganglionitis." It is clear from Hunt's own papers that multiple cranial nerves may be affected and that, in such cases, the facial nerve and its ganglion are perhaps most commonly involved.
Auditory and vestibular disturbances are common findings in patients with herpes zoster oticus. However, the incidence of hearing loss differs in the cases reported in the literature, ranging from 7%, to 19.7% (9), to as high as 85% (10). In our study, the incidence of patients complaining of hearing loss was 20%, and the incidence of patients who showed audiological abnormalities was 63%. Patients with audiological abnormalities in speech frequency range could detect hearing disturbance, but in cases of isolated high frequency loss, the patients did not have auditory symptoms in general.
The presence of cochlear and retrocochlear patterns of hearing loss has been reported by various authors. Wayman et al. (10), in a respective study of 186 patients with herpes zoster oticus-only seven of whom were studied in audiological detail-recognized one patient with retrocochlear involvement, five with cochlear involvement, and one with both cochlear and retrocochlear involvement. Abramovich and Prasher (11), in another detailed audiological examination of 13 patients with herpes zoster oticus, used electrocochleography and brainstem evoked potentials in addition to classic audiological tests. Seven of the 13 patients with aural herpes zoster who demonstrated retrocochlear involvement could be classified as sensory, with some patients showing both sensory and neural signs. However, Kaberos et al. (4), studied 15 patients with herpes zoster oticus through the use of otoacoustic emission in addition to auditory brain-stem response and demonstrated retrocochlear involvement in eight patients. Only three patients had purely retrocochlear hearing loss; the other five patients had concomitant cochlear involvement.
In our study, we were unable to demonstrate the cochlear or retrocochlear patterns by using only pure tone audiometry, but the audiological patterns of 111 patients among 160 patients with herpes zoster oticus were found to be less likely to be purely cochlear. The reason for the different incidence of high frequency hearing loss after onset of facial palsy might be explained by one of the cochleovestibular mechanisms in herpes zoster oticus: inflammatory changes throughout perineural tissues within the internal auditory canal and the peripheral and central cochlear nerve, and inflammatory changes in the cochlear nerve from the basal to apical turn.
The ears of elderly patients are more vulnerable to VZV compared to those of younger patients, especially in isolated high frequency (with the elimination of possible presbycusis), according to our data. This could be explained by an age-related decline in VZV-specific cell-mediated immunity (12).
VZV-specific immune responses may play a direct role in limiting reactivation and the frequency and severity of herpes zoster and its complications observed in elderly persons. There is an age-related decline in cell mediated immunity to VZV (13) (during most VZV reactivation events, the immune system is capable of neutralizing viral migration to neighboring cells).
In our study, the incidence of vestibular dysfunction in patients with herpes zoster oticus increased as severity of facial paralysis increased, while that of cochlear dysfunction did not. This could be explained through anatomical features of the vestibular-facial connection in the internal auditory canal. While direct connection between the facial nerve and cochlear nerve has not yet been found, it could be projected that viral spread though direct nerve fiber, not through perineural, invasion may lead to more severe dysfunction to the endorgan. Therefore, mild or moderate auditory symptoms and severe vestibular symptoms in general may be attributed to viral transmission across the perineural tissues between the facial nerve and cochlear nerve and to its spread through the superior vestibular-facial connection inside the internal auditory canal (14). Although the connection and spatial orientation in the internal auditory canal is not fully understood and has not been extensively studied, the connections between nerve fiber bundles are thought to be important in viral transmission, resulting in vestibulocochlear nerve disease in patients with herpes zoster oticus.
CONCLUSION
The results of this study support the thesis that viral spread from the geniculate ganglion to the eighth nerve through the perineural sheath, and the connection between nerve fiber bundles in the internal auditory canal, are important factors in vestibulocochlear nerve disease in herpes zoster oticus. Clinical impact of herpes zoster could be magnified by age-related suppression in cell-mediated immunity.