INTRODUCTION
In pediatric patients, the estimation of endotracheal tube (ETT) size is still controversial. Anatomical, structural, and developmental investigations have resulted in age-, height- and weight-based associations with developmental and structural alterations in the pediatric airway [1-3]. In terms of airway management, ETT size estimations still require methods that allow rapid and accurate decisions.
The most rapid method for the determination of ETT size in pediatric patients depends on age. Age-based recommendations are used in infants and children. More specifically, the Cole formula [inner diameter of ETT=(age/4)+4] is recommended for children >2 years (>24 months) of age [4]. The Cole formula has been reported to have a correct prediction rate of 47%–77% [5-7]. Height-based estimations such as the Broselow tape and formulas including height, weight, and age have been utilized [6,8,9]. However, such formulas have been suggested to be of limited use due to a lack of estimation for individual variations in the growth of internal organs [6].
The growth of children is assessed by considering both weight and height and their correlated increase with age. The percentile charts for weight-for-age and height-for-age are used to monitor growth. Children who are at <5% for weight-for-age and height-for-age may have smaller tracheal dimensions with respect to their age. Therefore, the Cole formula may be more misleading in these children. Despite the limitations of their study, Daugherty et al. [10] investigated children with pathologically short stature (PSS; <5% height-for-age) for the estimation of correct ETT size, and reported that height-based predictions were at least as accurate as age-based predictions in both PSS and normal children [10]. A more precise method including both weight and height for the assessment of the growth of a child involves calculating the body surface area (BSA) [4]. In our study, BSA was investigated for its advantage of including two major parameters (weight and height) that are used to monitor growth in children. In a recent study, Neunhoeffer et al. [11] created new diagrams based on BSA to predict the correct tube length and reported that the rate of correction for the placement of an ETT decreased after employing these diagrams. In investigations addressing the structure of the pediatric airway, the transverse diameter of the subglottic region was reported to be the narrowest of all regions and was found to be positively correlated with the height and the cross-sectional areas of both the glottis and the cricoid, which were found to be positively correlated with age, height, and weight [2,3]. In addition, the cross-sectional area of these two regions was reported to closely approximate each other with increasing growth [3]. Considering these data and the non-linear increases in height, weight and surface area in children with respect to age, we thought that the tracheal dimensions may be affected by individualized growth and the speed of that growth. Therefore, to include the main parameters that are used to monitor the growth of a child, we aimed to determine the impact of BSA on the correct outer diameter of an appropriate uncuffed-endotracheal-tube (ETT-OD) compared to the age-based Cole formula.
In recent years, ultrasound has proven to have a higher rate of prediction of the correct ETT size in pediatric patients than any other frequently used methods [5-7]. Our first objective was to investigate the association between the outer diameter of the correct ETT and BSA in a group of pediatric patients between 24 and 96 months of age. Our second objective was to determine the associations between age, height and weight as predictors of the outer diameter of the correct ETT and to determine whether percentiles of weight- or height-for-age have an impact on tube exchanges. Our third objective was to compare the associations between the Cole formula, BSA and the ultrasound measurement of the transverse diameter of the subglottic area with the correct ETT size in subgroups by age in patients aged 24–96 months.
MATERIALS AND METHODS
After obtaining approval from the Institutional Ethical Board Committee (No. 14/124-12; 30.04.2014) and written informed parental consent, 24 to 96-month-old American Society of Anesthesiology (ASA) physical status grade I–II patients, undergoing elective surgical procedures (for which endotracheal intubation was indicated) between March 1, 2016 and August 31, 2016 (6-month period) were examined for study purposes. Patients with known or suspected laryngeal or tracheal pathologies or syndromes characterized by airway anomalies or difficult airways were not included. Data on age (years and months), body weight and body height (measured the day before surgery) were obtained from records and BSA was calculated using the Mosteller formula {BSA (m2)=√[weight (kg)×height (cm) 3,600–1]} [12]. Percentiles pertaining to weight- and height-for-age were determined using growth charts (Centers for Disease Control and Prevention [CDC 24/7]) [13].
All patients received standardized anaesthetic management. All patients received oral/nasal administration of 0.5 mg/kg midazolam. Electrocardiography, noninvasive blood pressure, and peripheral oxygen saturation were monitored. Anaesthetic induction was provided by sevoflurane. After obtaining intravenous access, 1 mg/kg of propofol and 1 μg/kg of fentanyl were administered and 0.6 mg/kg rocuronium was used for muscle relaxation.
Ultrasound measurements (40 mm linear probe, 12-7 MHz; Titan, Sonosite, Bothell, WA, USA) were performed before intubation and after obtaining paralysis. The probe was first used to locate the hyoid cartilage, which was then moved caudally to locate the true vocal cords, and the subglottic transverse diameter was obtained immediately below the vocal cords. The measurements were performed by briefly interrupting positive pressure ventilation (without positive end-expiratory pressure) to minimize alterations in airway diameter for less than 30 seconds. The measurements were performed by the same anaesthesiologist (FU) after a supervised learning period. Endotracheal intubations were performed using direct laryngoscopy and an uncuffed ETT, and the tube sizes were determined using the Cole formula: inner diameter (ID)=(age [years]/4)+4. The ETT sizes were as follows: (ID/OD)=4.0/6.1, 4.5/6.6, 5.0/7.1, 5.5/7.7, and 6.0/8.4 mm (Bicakcilar, Istanbul, Turkey). If the tube size obtained from the Cole formula was between two sizes, then the smaller tube was selected. During the first attempt, if resistance was encountered, the tube was exchanged for a tube that was 0.5 mm smaller. The depth of the tracheal tube was confirmed by auscultation, and ventilation was examined via tracheal leak. Respiratory pressures were slowly increased (provided that the pressure did not exceed 25 cmH2O) to identify an audible leak from the patient’s mouth. If there was an audible leak with an airway pressure <10 cmH2O, the tube was exchanged for one that was 0.5 mm larger. If there was no leak with a pressure >20 cmH2O, the tube was exchanged for one that was 0.5 mm smaller. An audible leak between 10 and 20 cmH2O was only acceptable if ventilation was adequate. Otherwise, if the leak was excessive and did not allow adequate ventilation with plateau-type end-tidal capnography, the tube was exchanged for one that was 0.5 mm larger. In patients who had an excessive air leak with an uncuffed tube with an ID of 6.0 mm (OD, 8.4 mm), the tube was exchanged for a cuffed tube with an ID of 6.0 mm instead of exchanging with an uncuffed tube with an ID of 6.5 mm. Because uncuffed ETTs are not preferred in children over 8 years of age, for which the Cole formula concludes on an uncuffed ETT with an ID of 6.0 mm. Therefore, patients who needed an uncuffed ETT with an OD larger than 8.4 mm (ID, 6.0 mm) were intubated with a cuffed ETT with an OD of 8.4 mm. These patients were excluded from the correlations with size and were included in the analyses of tube-exchange rates and size estimation rates. The correct uncuffed ETT sizes for these patients were accepted as OD >8.4 mm for estimation rates. Since the inflated cuff would not reflect the exact size, these patients were not included in the analysis for correlations with size. The correct tube outer and inner diameters (correct ETT-OD and ID) and the tube exchanges were recorded. If an ETT was exchanged more than twice, 1 mg/kg of intravenous methylprednisolone was administered. Ultrasound measurements and examinations for tracheal leak were performed with the patient in the supine position with the head and neck in neutral position.
The Cole formula was compared to the correct ETT-ID because the formula estimates inner diameter. Similarly, because ultrasound measures the tracheal diameter to fit the outer diameter of the ETT, comparisons were performed using the correct ETT-OD. All correlations were performed using the correct ETT-OD. Considering that adequate ventilation is provided by a sufficient seal that is established by the tracheal mucosa and the ETT, a sufficient seal depends on the outer diameter of the ETT. Moreover, outer diameter matched inner diameter changes depending on the manufacturer. Therefore, the outer diameter was used for the correlations.
The subgroups of age were determined in terms of months: ages ≥24 to <48, ≥48 to <72 and ≥72 (≥72 to ≤96) months. The groups were determined according to the tube sizes estimated by Cole formula; 24 months of age (2 years), 48 months of age (4 years), 72 months of age (6 years) and 96 months of age (8 years) were to be intubated with ETTs of internal diameters of 4.5 mm, 5 mm, 5.5 mm, and 6 mm, respectively. Hence, there were only two size possibilities for each subgroup. If the age was in between according the tube size, we preferred the smaller tube as mentioned before.
The primary aim of this study was to determine the effect of BSA on correct ETT-OD. A total sample size of 102 was required to detect the correlation between BSA and ETT-OD after adjusting for age with a power of 95% at a 5% significance level. The sample size estimation was performed using G*Power ver. 3.0.10 (Universitat Kiel, Kiel, Germany). After calculations for drop-out, a sample size of 127 was defined.
Statistical analyses
Descriptive statistics are shown as the number of cases and percentages for categorical data. The mean±standard deviation or the median percentiles (25th–75th) were used for continuous variables. Whether the mean differences between clinical measurements were statistically significant was evaluated with a paired sampled t-test. Degrees of association between continuous variables were tested using a Pearson moment correlation analysis. Bland-Altman plots were used to assess the magnitude of the disagreement between the correct ETT-OD and ultrasound measurements and between the correct ETT-ID and the Cole formula. The means of agreement differences (i.e., bias) and the lower and upper limits set at a 0.95 confidence interval were also calculated. The maximum allowable deviation of the measurements from the correct ETT-OD or ID was ≤0.3 mm [5]. Univariate linear regression analyses were applied to determine the effect of each independent variable on the correct ETT-OD. Coefficients of regression, 95% confidence intervals and t-statistics for each independent variable were also calculated. The differences in estimation rates (i.e., under-, correct- and over-estimates) between indicators (i.e., Cole formula vs. BSA and Cole formula vs. ultrasonography were analyzed by the McNemar test. The data analysis was performed by using MedCalc ver. 11.1.1.0 (Broekstraat 52, B-9030; MedCalc software, Ostend, Belgium). A P-value less than 0.05 was considered statistically significant.
RESULTS
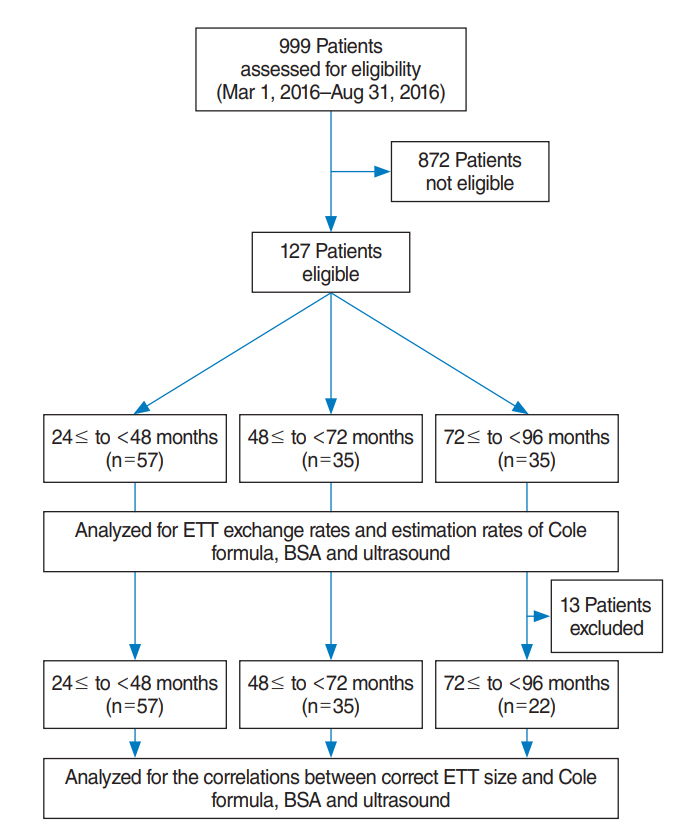
In this study, we evaluated 127 patients who were 24–96-months old, with ASA grades of I–II, who were scheduled for surgical procedures in which endotracheal intubation was indicated. A total of 13 patients required an ETT with an ID larger than 6.0 mm and were intubated with a cuffed ETT with an ID of 6.0 mm. These patients were in the ≥72 to ≤96 months age group and were excluded from the size analysis but have been presented as percentages in size estimation rates. The data of 114 patients were included in the size analysis (Fig. 1). Demographic data are shown in Table 1. The correct uncuffed ETT-ODs used are shown in Table 2. The most frequently used uncuffed ETT-OD for each subgroup of age is highlighted (Table 2).
In Table 3, the effects of weight (per 1 kg), height (per 10 cm) and BSA (per 0.1 m2) in each subgroup of age are given. All three parameters were effective for tube size estimation in all subgroups of age except for weight in children at the age of ≥48 to <72 months (P=0.119) (Table 3).
In all patients (age ≥24 to ≤96 months) and in all subgroups of age the correct estimation rates of the Cole formula, BSA and ultrasound were similar (Table 4). In ≥24 to <48 months age patients, the under-estimation rates of the Cole formula were higher (P=0.021) compared to BSA, but the under-estimation rates were similar with ultrasound (P=0.167). The over-estimation rates of the Cole formula were lower than both BSA (P=0.021) and ultrasound (P=0.002). In ≥48 to <72 months age patients, despite statistical insignificance, the under-estimation rate of the Cole formula (42.9%) was higher compared to both BSA (31.4%) and ultrasound (31.4%), but the correct estimation rates of BSA (37.2%) in this subgroup of age were lower than both the Cole formula (54.3%) and ultrasound (54.3%) (Table 4). In patients ≥72 months, the under-, correct- and over-estimation rates of the Cole formula, BSA, and ultrasound were all similar. However, the under-estimation rates were higher than in the other age sub-groups for all three parameters. The under-estimation rates of the Cole formula, BSA and ultrasound increased as the age of the children increased (Table 4).
The percentiles of weight- and height-for-age in our patient group were 0.50 (0.10–0.75) and 0.75 (0.25–0.90), respectively. The patients below 5% of weight-for-age and height-for-age were 17.5% and 8.8%, respectively. The tube-exchange rates did not reveal a significant correlation with weight percentiles (r=0.019, P=0.842) or height percentiles (r=0.123, P=0.194).
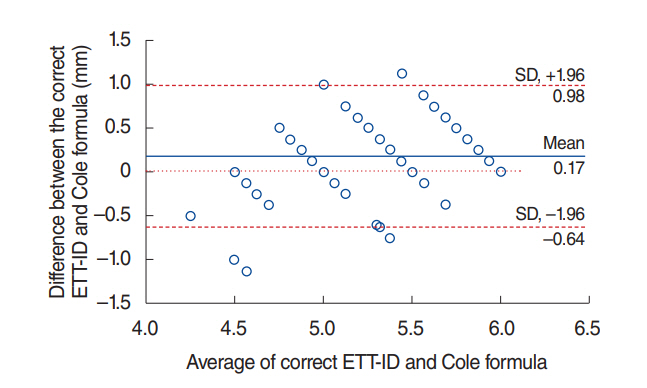
Tube size estimations using the Cole formula were lower than the correct ETT-ID by 0.17±0.41 mm (95% confidence interval [CI], –0.64 to 0.98) (Fig. 2) despite the significant positive correlation between the correct ETT-ID and the Cole formula (r=0.637, P<0.001). The 13 patients who were excluded from the size analysis also had unsuccessful predictions obtained from the Cole formula. When those patients were included, in 127 (114+13 patients) patients, tube-exchange rates by using Cole formula were as follows: the correct ETT was found during the first attempt without exchange in 44.9%, during the second attempt in 46.3%, and during the third attempt in 8.8% of patients. And the percentages in subgroups of age were obtained as follows: the tube size was correctly estimated by Cole formula during the first attempt in 29 patients at age ≥24 to <48 months (n=57, 50.9%), in 19 patients at age ≥48 to <72 months (n=35, 54.3%) and in nine patients at the age of ≥72 months (n=35, 22 uncuffed and 13 cuffed, 25.7%).
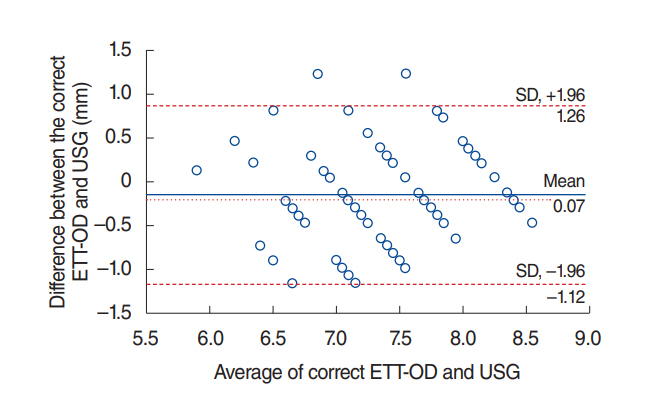
The ultrasound measurements were lower than the correct ETT-OD by 0.07±0.61 mm (95% CI, –1.12 to 1.26) (Fig. 3) with a significant positive correlation (r=0.499, P<0.001) even though the correct ETT-OD (7.35±0.58 mm) was found to be similar to the ultrasound measurements (7.42±0.63 mm) (P=0.221).
DISCUSSION
Our data suggested that BSA resulted in a similar prediction rate to the Cole formula for patients at age ≥24 to ≤96 months of age. Its correct estimation rate was 40.2% in all ages, indicating that it is not reliable for clinical use. Age, height, and weight were previously reported to positively correlate with pediatric airway dimensions and correct uncuffed ETT size, similar to our results [3,8]. Hofer et al. [9] reported that height-based ETT size estimation using a Broselow tape had a higher predictive value compared to age-based predictions [9]. In a similar study by Daugherty et al. [10], PSS (<5% of height-for-age) children were investigated for the comparison of two methods including age- and height-based formulas for the prediction of ETT size. The height-based estimation of the Broselow tape was comparable to the age-based formula in both PSS and normal children [10]. In our study, height also had a higher correlation with correct ETT size compared to age and weight. In addition, the exchange rates were not different in children <5% for both weight-for-age and height-for age.
The correct prediction rate of the age-based Cole formula has been reported to be 47%–77% [6]. In investigations addressing the Cole formula or other age-based estimations, Bae et al. [7] reported 31%, Schramm et al. [5] reported 24%, Shibasaki et al. [6] reported 60%, and Daugherty et al. [10] reported 43.2% for the correct prediction rates of age-based estimations. In those studies, infants and young children <2 years of age were also included, which may have constituted a confounding factor. In our study, we included a pediatric group of patients who were ≥24 months (≥2 years) of age for whom the exact Cole formula calculation is currently recommended for the prediction of uncuffed ETT size [4]. Our results also showed a similar rate of 44.9% for the Cole formula to predict the correct uncuffed ETT size. Moreover, the Cole formula had the lowest predictive value in patients ≥72 months of age.
The subglottic transverse diameter measured by ultrasound has previously been shown to have a higher predictive value for ETT size compared to age-based formulas [5-8]. Schramm et al. [5] reported a rate of 48%, Bae et al. [7] reported 60%, and Shibasaki et al. [6] reported 96% (despite the mean bias of 3.3 mm (1.9 to 4.6 mm). In Schramm et al.’s study [5], ultrasound measurements did not differ significantly from the correct tube size with a mean bias of –0.02 mm but were within the limits of agreement (–1.12 to 1.08 mm), which was similar to our study. Bae et al. [7] suggested an ultrasound-based estimation as a better alternative to age-based formulas, but it was not reliable for the prediction of appropriate ETT size. In our study, the predictive value of the ultrasound-based estimation was 42.5%, which was similar to previously reported data. Ultrasound may constitute a feasible technique for airway anomalies, but it is an operator-dependent technique, and the predictive value depends on experience despite the suggestion that it is an easy-to-learn technique [6,14]. Subcutaneous fat, probe pressure on the skin, and diagonal slicing may result in errors, but these can be overcome by experience. There are also some drawbacks despite reasonable experience: ultrasound is known to provide distance measurements as accurate as ±1 mm, which may become crucial in the prediction of the size of an ETT in children [8]. Ultrasound was shown to have a higher predictive value, but it was also reported to be useful only for uncuffed tubes [15].
In our study, in patients ≥72 months of age, 40% required an uncuffed ETT with an OD of 8.4 mm and 37.1% needed a cuffed ETT with an OD of 8.4 mm (Table 2). Therefore, we suggest considering either an uncuffed or cuffed ETT with an OD of 8.4 mm in patients who are ≥72 months of age. We can also consider using a cuffed ETT with an OD of either 7.7 or 8.4 since it is obvious that the Cole formula more frequently underestimates ETT size in patients over 72 months of age. Similarly, in patients who were ≥48 to <72 months of age, 31.3% required an uncuffed ETT with an OD of 7.1 mm and 65.8% (42.9% and 22.9%) needed a larger uncuffed ETT (Table 2). Either an uncuffed or cuffed ETT with an OD of 7.1 mm may be considered in patients who are ≥48 to <72 months of age. In patients who were ≥24 to <48 months of age, 52.6% needed an uncuffed ETT with an OD of 7.1 mm, 24.6% needed a 0.5 mm smaller ETT, and, 15.8% needed a 0.5 mm larger ETT. This patient group may be of clinical importance for future studies that examine BSA specifically to determine the actual correct uncuffed tube. However, it may also be suggested that either an uncuffed ETT with an OD of 6.6 mm or a cuffed ETT may be considered in this patient group because cuffed ETTs have also been recommended for small children given that cuff pressure monitoring is employed. These age subgroups and their relationship with BSA may lead to future studies.
There are some limitations to our study. Cuffed ETTs have been shown to be used safely in children. However, size estimation studies addressing cuffed tubes may overestimate the success rates of predictive techniques. If a technique predicts a smaller ETT than is actually necessary, the inflation of the cuff with appropriate pressure may overcome the problem concerning the incorrect size estimation. Therefore, in our study, we studied on uncuffed tubes. But, we also suggested using cuffed tubes for subgroups of age and tried to suggest their predicted sizes. However, we cannot suggest a definitive predictive technique.
We examined the otherwise healthy patients undergoing elective surgery. We did not do any test to rule out asymptomatic idiopathic or congenital subglottic stenosis. The most common cause of acquired stenosis has been reported to be prolonged intubation, whereas, congenital/idiopathic subglottic stenosis has been reported mostly to be associated with syndromes [16]. Hence, we assessed the history and the presence of syndromes related to any airway pathology and evaluated the presence of any symptoms regarding the airways in order to rule out any airway pathology. Fiberoptic bronchoscopy and imaging techniques are mainly the recommended techniques to rule out stenosis [17]. However, we did not use these techniques to rule out this rare condition. Ultrasound may have been beneficial but the measurement accuracy may differ ±1 mm, which may have misled our measurements. Moreover, in our study, the Cole formula and ultrasound measurements mostly underestimated the size of the tracheal tube, thus we do not think that our results may have been affected by the lack of assessment for stenosis. But, since there are few studies that examine the presence of asymptomatic idiopathic or congenital subglottic stenosis in children, addressing this parameter in future studies will be beneficial.
The high underestimation rate of the Cole formula may have been caused by our preference in favor of smaller size tube when the Cole formula concluded on a value between two sizes. There were nine patients for whom the Cole formula concluded on a size between two. Four of them were at 36 months of age and five of them were at 60 months of age. The tube sizes of three of four patients who were 36 months old and the tube sizes of three of five patients who were 60 months old were underestimated by the Cole formula. We think that the difference of underestimation rates between the age subgroups was not affected.
The correct estimation rates of Cole formula were low for all age groups that the percentages of endotracheal intubations at second and third attempts were to be applied. These second and third attempts may have caused swelling of the mucosa influencing our results. Eight patients at ≥24 to <48 months of age, one patient at ≥48 to <72 months of age and three patients at ≥72 to ≤96 months of age were overestimated by Cole formula, thus intubated with a smaller tube. We did not exert pressure to advance the ETT in case of resistance and since overestimation was detected to be low, we believe that our results were not affected.
The patients who required a larger ETT rather than an uncuffed ETT with an ID of 6.0 mm were intubated with a cuffed ETT with an ID of 6.0. Although there is no reason to prefer uncuffed tubes in children <8 years of age, this has long been known as the transition age for operator preference of cuffed or uncuffed tubes. Children who required a larger ETT than one with an ID of 6.0 mm (OD, 8.4 mm) were considered old enough to be intubated with a cuffed ETT, and intubation with an uncuffed ETT with an OD of 9.1 mm (ID, 6.5 mm) was not attempted. Instead, these patients were directly intubated with a cuffed ETT with an OD of 8.4 mm. We excluded these patients from the size analysis because we could not be sure of the actual diameter that fit. We believe that our results pertaining to the association between BSA and the uncuffed ETT-OD were not affected by this exclusion.
We addressed the use of BSA for tracheal tube size estimation. The predictive values of either height or age alone are known to be low. We thought that the growth of children, which is evaluated by BSA may also be of use in predicting tracheal tube size. The growth of children is also evaluated by percentiles of weight-for-age and height-for-age. However, we did not find a higher success rate for BSA in predicting ETT size or any correlation between tube exchange rates and growth percentiles. Weight may constitute noise rather than a signal but should be evaluated for its effect on predicting the appropriate size of uncuffed ETT, especially in children with growth retardation defined as <5% of weight-for-age.
Ultrasound measurements were performed at the subglottic level immediately below the vocal cords cephalad to the cricoid cartilage. The subglottic area has been defined as the distance between the vocal cords and cricoid cartilage [1,2]. The transverse diameter of this subglottic area was reported to be the narrowest dimension of the airway in children, proving that the contour of the airway in infants and children is different from the previously postulated cone shape [1,2]. The length of this area is difficult to focus on within the ultrasound beam, which may have caused lapse in measurements. In addition, any test-retest reliability measurements were not performed. As an operator-dependent technique the ultrasound measurements become more reliable as the experience of the user increases, which may have lowered the successful prediction rates in our study. However, our results were consistent with the results of most previous studies.
We could not present data for postextubation airway complications because they were not an outcome parameter. However, we did not encounter airway complications that required interventions or nebulized steroid therapy. This might have been solved with the 1 mg/kg of intravenous methylprednisolone administered to our patients who required a tube exchange more than twice. BSA estimated the correct uncuffed ETT-OD successfully at a rate of 40.2% in patients between age ≥24 and ≤96 months. The BSA, Cole formula, and ultrasonography revealed similar estimation rates. All three parameters had their lowest estimation rates in patients between ≥72 and ≤96 months of age.